An Introduction to This Antiphospholipid Syndrome Resource Guide
If you've just received an Antiphospholipid Syndrome diagnosis, you're probably unsure of where to start, and might be a little frightened by the prognosis. I was the same when I was first diagnosed with Antiphospholipid Syndrome (APS) at 14, and subsequently developed DVTs (deep vein thrombosis) and a Pulmonary Embolism (PE) at 17. There may be some information about Antiphospholipid Syndrome from medical sources online, but patient tips, stories and life experiences are fairly lacking.
For those of you who’ve never heard of Antiphospholipid Syndrome (APS), I don’t blame you. It’s a rare blood clotting disorder that's seldom discussed in the media. It did get a little bit of limelight during the pandemic, as COVID patients suffered from hypercoagulation as a symptom (van der Linden, 2020). Although it’s an autoimmune disease that affects the blood, Antiphospholipid Syndrome can manifest in other parts of the body such as the brain, lungs, heart, kidneys, gastrointestinal system, and more (Gezer, 2003).
This is an A to Z guide for those with an Antiphospholipid Syndrome diagnosis. Over time, I aim to build up more resources about APS, with this serving as a main reference page. Let me know if you think I’ve missed anything out, or if something should be added in or amended. Let's work together to make this a useful patient resource!
*Disclaimer: This blog and page is meant for educational purposes, and is based on my personal experiences as a patient. I am not a doctor, and nothing on this website should be substituted for medical advice. Please consult your own doctor before changing or adding any new treatment protocols. This page may also contain affiliate links. It will cost you nothing to click on them. I will get a small referral fee from purchases you make, which helps with the maintenance of this blog. Read our Privacy Policy page for more information. Thank you!
-
Changelog:
- 23 May 2025: Replaced link from Penn Medicine (2022) to Jaffer and Bragg (2003) as the previous link is no longer available.
- 17 Jan 2025: Replaced link from Dickmann et al. (2001) to Lindley et al. (2022) under “African Americans” section, as the previous paper is no longer available.
How to Use This Antiphospholipid Syndrome Diagnosis A to Z Guide
This guide can be read as standalone sections in any alphabetical order - just do a search or skip to whichever section you’re looking for keywords in. An alphabetical menu can be found at the end of each section for easier navigation.
I have separated certain topics into their own posts, such as medications, research and women's health, as they truly need an entire post of their own. I have included these links where appropriate. I am currently also doing research into APS and food, and plan to write a mini series that revolve around the topics of herbs, vegetables, diet and more. I will update this A to Z guide as we go along, and you can find the changes in the changelog when I do.
Audio will be added over time and will be split up by alphabet, and can be found at the beginning of each section. If there are other accessibility features that you think might be helpful - just let me know in the comments section.
How to Support Me & My Advocacy Work
I have been working on this resource on and off over a few years. It truly is a work-in-progress, as there are still many related topics I’d like to include, and also to expand upon. But at some point, you need to just release it into the wild, whilst making improvements along the way - hopefully with other patient input and insights as well.
I have spent hundreds, if not thousands of hours on this resource guide, as well as other articles on this website. If you like what I do and would like to support me, you can buy me a cup of coffee (I do drink too much coffee, this is true 😉), or commit to a monthly contribution by signing up for a paid subscription!
Pin to Your Antiphospholipid Syndrome Diagnosis Boards:
A is for Antiphospholipid Syndrome, Anticoagulants & The 2023 ACR/EULAR APS Criteria
Antiphospholipid Syndrome
Well, of course we need to start with Antiphospholipid Syndrome (APS) itself! So what is APS, exactly? According to the National Heart, Lung, and Blood Institute (NHLBI) (2022a):
“Antiphospholipid syndrome (APS) is an autoimmune disorder that causes abnormal blood clots to form. Autoimmune disorders occur when your body’s immune system makes antibodies that attack and damage your own tissues or cells.”
Another surprising thing to note is that whilst APS is usually associated with blood clotting, sometimes it can also lead to bleeding. According to Ahluwalia and Sreedharanunni (2017):
"The bleeding may be related to severe thrombocytopenia, platelet function disorders, factor VIII inhibitor, prothrombin deficiency and rarely to acquired deficiency of factors VII, X and XI."
You can learn more about the systemic implications of Antiphospholipid Syndrome in this post.
Laboratory tests used to identify patients who have Antiphospholipid Syndrome are: anticardiolipin (aCL), and/or anti-β2GPI, and/or lupus anticoagulant (LA) assays. A laboratory test needs to be positive on at least two occasions, separated by 12 weeks, to be considered diagnostic for Antiphospholipid Syndrome (Gómez-Puerta & Cervera, 2014).
Anticoagulants
There are many types of anticoagulant medications, which work by preventing the blood from clotting (Cleveland Clinic, 2022a). In general, patients who have had thrombotic events before need to be on warfarin with an even higher target INR range.
This is a great paper that covers the different types of anticoagulants in detail (Nutescu et al., 2016), should you be interested to learn more. I have also written more about medications and drugs used in relation to APS in this post.
The 2023 ACR/EULAR APS Criteria
The 2023 American College of Rheumatology (ACR) / European Alliance of Associations for Rheumatology (EULAR) APS criteria consists of four phases. These include a combination of surveys, literature reviews, criteria reduction, criteria definition, and validation, with actual patient scenarios for guidance (Barbhaiya et al., 2023).
It was formulated to address some of the limitations of the previous Sapporo criteria(s), and serves to narrow the heterogeneity gap of patients who are positive for antiphospholipid antibodies (aPLs). The 2023 ACR/EULAR APS Criteria has an increased specificity compared to the 2006 revised Sapporo criteria (99% versus 86%), although it also has a lower sensitivity (84% versus 99%) (Barbhaiya et al., 2023). The 2023 ACR/EULAR APS Criteria still needs to be fully validated for some subsets of patients as well, such as Lupus patients who are positive for antiphospholipid antibodies (Koliadenko & Iaremenko, 2024).
According to Yang et al. (2024), who did a small study on a cohort of Chinese patients:
“Revisions to clinical criteria included refined risk stratification for venous thromboembolism (VTE) and cardiovascular disease (CVD), a clarified definition of microvascular thrombosis, a redefined understanding of pregnancy morbidity, and heightened consideration of cardiac valve disease and thrombocytopenia. The introduction of these new criteria helps identify patients who were previously only diagnosed as “probable APS”.”
Based on the 2023 ACR/EULAR APS criteria, Yang et al. (2024) were able to diagnose an additional 9 patients with Antiphospholipid Syndrome, in a cohort of 965 patients.
Classification vs Diagnostic Criteria
Favaloro et al. (2024) makes an emphasis on the importance of differentiating classification from diagnostic criteria as well:
“In other words, the “classification” criteria establish a finite list of clinical and laboratory parameters that can be used to identify some “definite” APS manifestation for inclusion in future studies, but a broader list of both clinical and laboratory criteria are available to help diagnose APS.”
..... “Therefore, diagnostic criteria are a set of signs, symptoms, and tests for use in routine clinical care to guide the clinical decision making in individual patients. Classification criteria are instead standardized definitions used primarily to create well-defined, relatively homogeneous cohorts of patients for clinical research.”
In short, the point that Favaloro et al. (2024) makes is that whilst APS diagnoses can be made by clinicians based on the most recent 2023 ACR/EULAR APS criteria, other APS manifestations should be taken into consideration as well. This is especially crucial when the patient presents with non-criteria APS manifestations.
Some other keywords under ‘A’ and APS are:
-
Acute Pain - A blood clot or haemorrhage can be cause for acute pain anywhere in the body, and I've had the misfortune of experiencing both on numerous occasions. These events can be life-threatening and require immediate medical attention. Head to the A&E/ER right away even if you're unsure of the exact cause, and never 'wait it out' - this was my biggest regret in life.
-
Alcohol - People who have recently received an Antiphospholipid Syndrome diagnosis often wonder if they can still drink alcohol (Caporuscio, 2021). Usually a maximum of two glasses of alcohol is allowed, as alcohol is a blood thinner that stays in the bodily system for a short duration of time (Hull et al., 2024; Thomas, 2024).
Having said that, this does not take into account your specific comorbidities, risk factors, liver function, medication interactions and more. So please check with your own doctor first before consuming alcohol.
There have also been studies that show associations with alcoholic liver disease, and the development of antibodies targeting complexes between oxidised cardiolipin and β2-GP1, which might account for higher levels of antiphospholipid antibodies in the individual (Rolla et al., 2001).
-
African Americans – In relation to the CYP2C9 gene, which plays a role in warfarin metabolism, it has been noted thus far that the CYP2C95 allele has been found in 5 out of 110 African-American APS patients, and CYP2C96 in around 0.6% of African-American APS patients as well. Neither have been yet found in Asian or Caucasian patients (Takahashi & Echizen, 2003).
And according to Lindley et al. (2022), “The cytochrome P450 2C9*5 (CYP2C9*5) allele is found almost exclusively in populations of African ancestry, and in vitro studies suggest CYP2C9*5 is associated with reduced clearance of warfarin”. What this means is that carriers of this genetic variant may require more warfarin than average. More investigation is still required, however, in order to determine its exact effects and functionalities.
-
aGAPSS - The Adjusted Global AntiphosPholipid Syndrome Score (aGAPSS) was developed to identify high-risk APS patients, and consists of: hyperlipidaemia (3 points), arterial hypertension (1 point), anticardiolipin antibodies (5 points), anti-β2 glycoprotein-I antibodies (4 points), and lupus anticoagulant (4 points) (Radin et al., 2019).
-
Alternative Therapies - I don’t deny the usefulness of holistic approaches to health and wellness, and some alternative and complementary therapies can be useful when adapted to an individual. Having said that, people who have an Antiphospholipid Syndrome diagnosis need to be cautious of such therapies, because many of them involve touch or dietary changes, which can lead to bruising and bleeding. These include massages, chiropractic adjustments, herbs and more.
-
Andexanet Alfa - This is a factor Xa protein used to reverse the effects of apixaban and rivaroxaban (blood thinning drugs used by patients), during life-threatening situations where there may be uncontrolled bleeding (Reed et al., 2023). Learn more about Factor Xa and Andexanet Alfa here.
-
Anti-Beta2 Glycoprotein 1 (anti-ß2 GPI) - Beta-2-Glycoprotein I (β2GPI) is a soluble blood protein, and has many functions, including haemostasis (blood clotting process).
According to McDonnell et al. (2020):
“Indirectly, β2GPI can exert an anticoagulant effect through downregulation of thrombin generation whilst its indirect coagulant effect is shown through mechanisms including inhibiting activation of protein C and disrupting the anticoagulant Annexin V shield.”
APS patients present antibodies, such as anti-ß2 GPI, that can dysregulate this process. Two isotypes found in anti-β2 GPI – IgG and IgM – are one of the diagnostic criteria for an Antiphospholipid Syndrome diagnosis. Whilst the IgA isotype is not currently used for diagnosis, there has been growing interest and research in it, especially for seronegative APS patients. In one study, there was a strong association for IgA and arterial thrombosis (Murthy et al., 2013). Learn more about thrombin and the coagulation cascade here.
-
Anticardiolipin Antibodies - Cardiolipins are phospholipids, and antibodies produced against them can lead to blood clots (University of Rochester Medical Center [URMC], n.d.-a).
Whilst research on antiphospholipid antibodies (aPLs) in relation to COVID-19 are still underway and not fully understood, interestingly, anticardiolipin antibodies (aCLs) have shown some correlations. Having said that, it is important to note that infections in themselves can also trigger a rise in antiphospholipid antibodies, and the pathways of blood clotting might differ from that of a patient who actually has an Antiphospholipid Syndrome diagnosis (Bertin et al., 2022).
-
Antiphospholipid Antibodies - The lupus anticoagulant, anticardiolipin and anti-ß2GPI antibodies are collectively referred to as antiphospholipid antibodies. Note that this is different from the autoimmune disease, Antiphospholipid Syndrome, itself. According to Green (2022):
These antibodies attack cells, cellular receptors, and hemostatic proteins either alone or in complexes with phospholipid-binding proteins.”
This triggers a sequence of events that can lead to a blood clot. About 50% of Systemic Lupus Erythomatosus (SLE) patients also possess antiphospholipid antibodies (Johns Hopkins Lupus Center, n.d.-b).
-
Antiplatelet Drugs - These are used to prevent platelets from sticking together, which decreases your body’s ability to form blood clots. Aspirin is one of the most commonly used antiplatelet drugs. These work differently from anticoagulants, even though they both prevent blood clotting. As per Cleveland Clinic (2022c):
“Antiplatelets interfere with the process of platelets binding together. Anticoagulants, also called blood thinners, interfere with proteins in your blood that are involved with clotting.”
For a more in-depth explanation, read this post on medications and Antiphospholipid Syndrome.
-
Antiphosphatidylserine / Prothrombin Antibodies - Studies have shown the correlation of antiphosphatidylserine / prothrombin (aPS/PT) antibodies with a higher association of clinical manifestations of Antiphospholipid Syndrome, and that it can be considered as a robust test for further investigation in patients with suspected APS (Radin et al., 2020).
-
Apixaban (Brand Name: Eliquis) - This is a direct oral anticoagulant (DOAC) originally approved for atrial fibrillation (Afib) patients to reduce the risk of strokes and blood clots. It was later approved to treat DVTs and PEs (pulmonary embolisms) as well (Agrawal et al., 2024). Learn more about apixaban and DOACs here.
-
Asians - According to Takahashi and Echizen (2003):
“Anecdotal observations indicated that the maintenance doses of warfarin obtained from Asians (ie, 3.4 and 3.3 mg/day for Japanese12,13,14 and Chinese,32 respectively) are 20–50% lower than those obtained from Caucasian (ie, 4.1–6.7 mg/day).”
This may be due to the fact that the Asians in the study did not possess the CYP2C9*2 variant, which is more commonly found in Caucasian populations. This variant, and also the CYP2C9*3 variant, both contribute to decreased metabolism of warfarin.
-
Aspirin / Acetylsalicylic Acid - This is an NSAID (which all have anticoagulatory effects), and some patients take it for other medical conditions such as heart problems. Aspirin is usually not strong enough of a blood thinner for those with Antiphospholipid Syndrome however, especially for those of us who have had DVTs and the likes before. It only reduces the risk of first arterial, but not venous thrombotic events in people with antiphospholipid antibodies (Pastori et al., 2021). Read this post for more information on NSAIDs, including aspirin.
Pin to Your Antiphospholipid Syndrome Diagnosis Boards:
B is for Blood Clots & Bleeding
Blood clots and bleeding are the bane of Antiphospholipid Syndrome. Either extreme can be cause for alarm, should they go out of control.
Blood Clots
The process of blood clotting is very important, as it helps your body to stop bleeding when you injure yourself, whether externally or internally. A blood clot is medically known as a ‘thrombus’, and a thrombosis is “a blood clot within blood vessels that limit the flow of blood” (Ashorobi et al., 2024).
Blood clots become dangerous when they break off to lodge in other places within the body, such as in the heart, brain or lung, and patients with Antiphospholipid Syndrome are at a higher risk (Mayo Clinic, 2023a). Many APS patients need to go on anticoagulation therapy in order to prevent blood clots, and are usually started on warfarin, a vitamin K antagonist. Patients who have experienced any blood clotting events before are usually medicated with a higher dose as well.
Bleeding
A little known fact is that APS patients can also bleed from the disease itself in rare circumstances. According to Kubisz et al. (2021):
"The acquired coagulopathy caused by the aPL, particularly by lupus anticoagulant and anticardiolipin antibodies, might be occasionally manifested as a hemorrhagic syndrome with various clinical severity."
And from Pazzola et al. (2015):
"Antiphospholipid antibody-positive patients can develop bleeding due to capillaritis, microthrombosis, antiprothrombin antibodies, thrombocytopenia, and/or excessive antithrombotic therapy."
Bleeding can range from mild to severe, and occur in various organs such as the brain or stomach. The interaction between antiphospholipid antibodies and the body is heterogeneous, with many possible factors at play. The management of APS during such events are even more complex, as both blood clotting and bleeding risks need to be managed.
Read about the systemic implications of APS in this post.
Other Terms for ‘B’ in Relation to APS are:
-
Birth Control - There are a few different types of birth controls, which mainly contain the hormones oestrogen, or progestin, or both. Oestrogen is known to cause blood clots, and is best avoided in all forms (Penn Medicine, n.d.). Whilst you may choose to be on birth control to prevent conception, sometimes women with APS need to go on them due to recurrences of ovarian cyst ruptures, which is a life-threatening event. Learn more about birth control here.
-
Blood Disorder - Antiphospholipid Syndrome is but one of many different types of blood disorders. You can view more blood clotting and bleeding disorders in this list from Cleveland Clinic (2022d).
-
Blood Tests - As with any other autoimmune disease and/or blood disorder, your doctor will monitor your blood closely for things such as inflammatory markers and full blood count. For patients with an Antiphospholipid Syndrome diagnosis, one of the most, if not the most important blood test is the one for PT/INR (International Normalised Ratio) (MedLinePlus, 2024).
-
Bone Loss - Long-term warfarin therapy can lead to bone density loss, as it antagonises vitamin K – an important vitamin for bone health (Rodríguez-Olleros Rodríguez and Díaz Curiel, 2019). Learn more about musculoskeletal manifestations here.
- Brain Fog - See Cognitive Function.
-
Broccoli - This may sound somewhat random, but I’ve personally found broccoli to be very high in vitamin K. Often 2 to 3 stalks of broccoli can drop my INR back down to baseline, so I balance this with blood thinning foods such as salmon carefully. Call it a food strategy.
-
Bruises - It’s easy to get bruises when you’re on an anticoagulant medication; it can be alarming especially in the beginning. It’s important to monitor all signs of bruising, especially the bigger ones. You will need to stop all contact sports, due to the high risk of bruising which increases the chances of DVTs.
-
Brushing Your Teeth - Ever brushed your teeth a little too hard and have your gums bleed? It’s best to use a toothbrush with soft bristles, or an electric toothbrush that has a sensitivity pressure warning. I’ve tried a couple and this is the electric toothbrush I currently use and like, as the price is decent, the bristles are small enough and it doesn’t clean with a vengeance.
Pin to Your Antiphospholipid Syndrome & Rare Disease Boards:
C is for Coagulation, Cardiovascular Disease & Catastrophic Antiphospholipid Syndrome (CAPS)
Coagulation
Coagulation is when the blood turns from a liquid to solid state and clots. Patients with Antiphospholipid Syndrome typically need to take anticoagulants to counteract their ‘sticky blood’, as they have an increased tendency to clot. The coagulation process is a fascinating one where lots of variables are at play, and one where researchers are still learning and discovering new things about even up to this day – such as the more recently known clotting factors – prekallikrein and high-molecular-weight kininogen.
According to Palta et al. (2014), clotting factors can be classified into the following three groups:
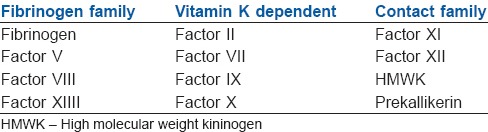 (Source: https://doi.org/10.4103/0019-5049.144643)
(Source: https://doi.org/10.4103/0019-5049.144643)
They also state that:
“Most of the procoagulants and anticoagulants are produced by liver except factor III, IV and VIII. These proteins undergo a post translational modification (vitamin K dependent ϒ carboxylation of glutamic acid residues) which enables them to bind calcium and other divalent cations and participate in clotting cascade. Deficiency of vitamin K or administration of vitamin K antagonists (warfarin) lead to anticoagulation.”
What this means in simpler terms is that the body produces both coagulants and anticoagulants on its own through various pathways internally, and that various proteins, elements and processes are involved in the coagulation process. It also means that altering vitamin K levels in the body, whether through the use of medications, or as a result of malabsorption or nutrient deficiency, can affect this process.
You can learn more about the blood clotting process in this post.
Cardiovascular Disease
Cardiovascular Disease (CVD) is a leading cause of mortality in Antiphospholipid Syndrome patients. On top of traditional risk factors, they also have thrombotic and inflammatory risk factors to contend with. Learn more about cardiovascular disease and APS here.
Catastrophic Antiphospholipid Syndrome (CAPS)
Catastrophic Antiphospholipid Syndrome is a rare occurrence that only occurs in 1% of APS patients, but is also the most severe manifestation of APS. It has a high mortality rate, especially if the patient has an SLE (Lupus) comorbidity. CAPS happens when multiple blood clots occur simultaneously throughout the body, which can lead to multiple organ, system and tissue failure (Cervera et al., 2018). Little is understood about the condition, although it is hypothesised to be multifactorial in aetiology, with genetic and environmental factors thrown in for good measure (Rodriguez-Pintó et al., 2024).
CAPS mostly affects women at 70%, and those who are in their forties, although it can occur at any age. Pulmonary (lung) manifestations, such as lung thrombosis and diffuse alveolar haemorrhage, occur in approximately two thirds of cases. Central nervous system (CNS) manifestations include strokes and encephalopathy, and occur in up to 56% of CAPS patients. Cardiovascular manifestations such as heart attacks and anginas can also happen, and is reported in approximately half of CAPS patients. And wait we aren’t done yet….. Skin manifestations such as livedo can also be found in 47% of CAPS patients, and it can also affect the liver, spleen, adrenal glands, reproductive organs, and just about every body part you can think of, I reckon (Rodriguez-Pintó et al., 2024).
The CAPS Registry was created by the European Forum on Antiphospholipid Antibodies, and contains a grand total of 500 CAPS patients. Rodríguez-Pintó et al. (2016) did a study on the demographics data, and found some common precipitating factors for CAPS to be events such as: infections, surgeries, malignancy, contraceptive use, pregnancy, drug use, SLE flares, trauma and more.
For more information, read the post, “How Does Antiphospholipid Syndrome Affect The Body? (Beyond the Blood to Major Organs)”.
Other Terms for ‘C’ in Relation to APS are:
-
Calcium -Calcium is the most abundant mineral in the body that is needed for various functions, including bone health. Our bodies also ‘borrow’ calcium from our bones should there be a deficit, which can lead to osteoporosis (National Institute of Arthritis and Musculoskeletal and Skin Diseases [NIAMS], 2023).
Warfarin is a Vitamin K antagonist (VKA) that affects bone health, so calcium is generally prescribed for Antiphospholipid Syndrome patients to help counteract this. Something to bear in mind is that many calcium supplements sold over-the-counter (OTC) are combined with vitamin K, as they have a synergistic effect. Do ensure that you read carefully through the ingredients, as these can interact with warfarin.
Read this post for more information on vitamin K antagonists and warfarin, and this post for musculoskeletal manifestations of APS.
-
Caucasians - According to MedLinePlus (2018):
“The two most common CYP2C9 polymorphisms in people of European ancestry are known as CYP2C9*2 and CYP2C9*3. Both of these polymorphisms lead to a decrease in warfarin metabolism to such degrees that prescription doses are typically reduced by one-third and one-fifth, respectively.”
What this means is that patients of European descent tend to require a lower dosage of warfarin, if they possess these polymorphisms.
-
CBD (Cannabidiol) - Can you take CBD whilst on warfarin? According to Grayson et al. (2018):
“In addition to competing for enzymes in same metabolic pathway as warfarin, CBD has been demonstrated to act as a potent competitive inhibitor of all seven of its own CYP enzymes and as such could further impair the degradation of warfarin.”
What this means is that there is a potential for CBD to interact with warfarin and cause bleeding. Thus, if it’s legal where you are and you want to take CBD, work with your doctor to monitor your INR.You also need to be consistent in intake, which sort of defeats the purpose – pain levels can fluctuate like the weather in Rapid City, South Dakota (yes I diverged to look that up 😜) (Silver & Fischer-Baum, 2014). There are also a lot of variations in CBD oils and products, which do different things in the body.
Read this post for more information about warfarin and medication interactions.
-
Chinese Patients - In a study of 252 Chinese APS patients, whilst common thrombotic events were found to be similar to those from the Euro-Phospholipid Project, lower positive rates of anticardiolipin and lupus anticoagulant antibodies were also found comparatively (Shi et al., 2017).
Asians in general also do not possess a certain allele for the CYP29C gene, which means they may require a lower maintenance dose of warfarin, as compared to caucasians. Having said that, a systematic review and meta-analysis that studied 20 single nucleotide polymorphisms in eight genes also revealed that other polymorphisms play a role in the mean daily warfarin dose of Chinese Han patients (Zhao et al., 2023).
- CoaguChek® - See Roche.
-
Cognitive Function - An impact in cognitive function is preferable to saying ‘brain fog’, which often makes the experience sound overly trivial. Those who live with ‘brain fog’ know how devastating its impacts are. Cognitive dysfunction is also another annoying feature of APS involvement in the neurological pathways, and exists on a spectrum from mild to severe (such as dementia) (Yelnik et al., 2016).
The frequency of cognitive dysfunction ranges from 19% to 40%, and includes cognitive complication with memory, executive function, visuospatial skills and visuomotor speed. APS patients can also present with psychiatric symptoms such as: psychosis, mania, depression, bipolar disorders, OCD and schizophrenia (Yelnik et al., 2016). You can learn more about the neurological manifestations of APS here.
-
Comorbidities - Patients with an autoimmune disease tend to have comorbidities, meaning that they have more than one medical condition at the same time (Cojocaru et al., 2010). The overlap of these comorbidities can be complex and more often than not, patients live with chronic pain whilst waiting for proper diagnoses.
-
Compression Clothing & Devices - If you’re stuck in bed or in a single position (such as on a flight) and can’t walk or move for a period of time, then wearing compression stockings and clothing can help to prevent the formation of blood clots.
APS patients tend to need to wear compression stockings after undergoing major surgery where they’re unable to walk about. An intermittent pneumatic compression device is also usually used when APS patients undergo surgery that requires general anaesthesia. These are cuffs that are wrapped around your legs which inflate and deflate to help with blood circulation (Cleveland Clinic, 2023b).
You can find some of my recommendations for compression clothing here, and check out my top tips for travelling with chronic illness and disability in this post.
-
COVID-19 - As mentioned in the introduction, many COVID-19 patients suffer from hypercoagulation. Whilst they may not have the APS disorder itself, greater than 80% had detectable antiphospholipid antibodies in their bodies (van der Linden et al., 2020).
It is important to note that research into antiphospholipid antibodies (aPLs) and COVID-19 is still preliminary, with the need for standardisation across various research methods. At present, it is generally accepted that the presence of aPLs in COVID-19 patients could be a secondary symptom of the infection, with each as contributing risk factors for thrombosis (Serrano et al., 2022).
In one study of 56 patients in France, 45% of them tested positive for the lupus anticoagulant (LA) (Harzallah et al., 2020). Many also experience a prolonged aPTT time, which is an indicator of a blood clotting deficiency, and up to 91% of such patients tested positive for LA in another study (Bowles et al., 2020).
You can find out more about the latest Antiphospholipid Syndrome research in this post.
-
Coumarin - Coumarins are naturally occurring compounds derived from 1,2-benzopyrone. They were first discovered in tonka beans, but can also be found in other plant products such as cinnamon, strawberries, green tea, lavender oil and more.
They are often used in perfumes and soaps in low quantities, as a stabiliser and fragrant ingredient. Although it is allowed for consumption via natural food products such as cinnamon, it is not allowed as a direct food additive due to its toxicity and anticoagulation effects (Garrard, 2014).
Warfarin is derived from coumarin, and is used to both kill rodents, and also as an anticoagulant drug for APS patients. The more science-y explanation, according to Lu et al. (2022):
“Coumarin-like drugs bind to vitamin K epoxide reductase complex 1 in the liver and block the conversion of inactive oxidative vitamin K into active reducing vitamin K. Active vitamin K is involved in the effects of coagulation factors II (reducing prothrombin production), VII, IX, and X.”
An interesting conclusion from the paper as well is that their results indicated that six of the tested coumarin derivatives inhibited ADP (adenosine diphosphate)-induced platelet aggregation, and also of calcium ions. Meaning, they target various coagulation pathways.
Learn more about warfarin drug interactions and vitamin K antagonists in this post.
-
Cupping, Traditional Chinese Medicine (TCM) & Chiropractor - These are just a few alternative therapies that aren’t such a good idea when you live with Antiphospholipid Syndrome. Many of the herbs that are used interact with warfarin (believe me, I’ve tried).
Cupping is a TCM treatment that works by drawing small amounts of blood through suction ‘cups’. Apart from those who have blood disorders, cupping is also contraindicated for many other patients such as those who have cancer, organ failure or an implanted electronic device (Furhad et al., 2023).
I asked my rheumatologist about visiting a chiropractor, and to my surprise, it wasn’t my Lupus or Sjögren’s that he was worried about, but Antiphospholipid Syndrome. Even if the manipulations were to be gentler, it can still cause blood clots or minor injuries.
-
CYP2C9 Gene - CYP2C9 Gene – The CYP2C9 enzyme plays a major role in the metabolism of warfarin, and other drugs such as ibuprofen. Polymorphisms can lead to an increase or decrease in warfarin metabolism (MedLinePlus, 2018, September 1).
According to Takahashi and Echizen (2003):
“Collectively, it is suggested that patients with CYP2C9 variants, particularly CYP2C9*3 allele or a combination of CYP2C9*2 and CYP2C9*3 alleles would be vulnerable to above-range INRs, need more time to achieve stable warfarin dosing and longer hospitalization and have a higher risk of serious or life-threatening bleeding events than those with wild-type CYP2C9 genotype during the induction or dose-titration period of warfarin therapy.”
This means that certain patients who possess particular variants of the CYP2C9 gene might have an increased risk of bleeding whilst on warfarin, and also take longer period of time to achieve their target INR range. Learn more about warfarin metabolism here.
Pin to Your Antiphospholipid Syndrome Diagnosis & Health Boards:
D is for DVT, Diet & Dermatologic Manifestations
Deep Vein Thrombosis (DVT)
DVT stands for ‘Deep Vein Thrombosis’, and they can be an extremely painful consequence of Antiphospholipid Syndrome. These blood clots tend to form in a deep leg vein, but can occur anywhere in the body. If they are large enough, they can lodge in the lungs, brain or heart, and that can turn into a life-threatening situation (Reyes & Abe, 2023). Learn more about DVTs and other manifestations of APS in this post.
Diet
The APS diet is the biggest and most confusing thing to contend with when a person receives an Antiphospholipid Syndrome diagnosis. Questions that pop up include: “Is that safe to eat whilst on warfarin?”, and “You mean I can’t eat or drink my favourite food stuff anymore?!”
I’ve been there. I remember being terrified, as I didn’t know what I could or could not eat and drink anymore. Every APS patient can react differently to the same foods as well, so what works for one person may not for another. But don’t be like me and live in denial; I continued to consume green tea in copious amounts and played contact sports, because there wasn’t any pain initially – until there was.
It will take a while, even years, to learn what foods are safe for consumption after an Antiphospholipid Syndrome diagnosis. I promise that it gets easier though, as you start to know how to keep your diet balanced in terms of Vitamin K and blood thinning foods. It will even become intrinsic knowledge, where you can roughly estimate what the status of vitamin K is within your body, more or less. The Antiphospholipid Syndrome diet is also a behemoth topic that requires a post of its own, and one which I will cover in greater detail in future.
Dermatologic Manifestations
Cutaneous (skin-related) manifestations are common and may actually be the first signs of Antiphospholipid Syndrome.
According to Gibson et al. (1997):
“These include livedo reticularis, necrotizing vasculitis, livedoid vasculitis, thrombophlebitis, cutaneous ulceration and necrosis, erythematous macules, purpura, ecchymoses, painful skin nodules, and subungual splinter hemorrhages.”
I cover the topic of dermatologic manifestations in APS more comprehensively here.
Some Other Terms for ‘D’ & APS are:
-
Vitamin D - Vitamin D comes in various forms, such as D2 and D3. It works together with calcium to promote bone health. According to Harvard Medical School (2021a):
“Without enough vitamin D, the body can only absorb 10% to 15% of dietary calcium, but 30% to 40% absorption is the rule when vitamin reserves are normal.”
APS patients tend to have a greater vitamin D deficiency of up to 70% as well (Kello & Cho, 2023). Thus, it is quite likely that your doctor will prescribe some sort of vitamin D supplement, especially if you’re on warfarin. Read this post for more information on bone health.
-
Diffuse Alveolar Haemorrhage (DAH) - DAH is a small vessel vasculitis that damages the lung microvasculature (Stoots et al., 2019). It is a rare condition that can happen to APS patients, with a high mortality rate between 30.3% – 45.8%. Learn more about the pulmonary and vascular manifestations of APS here, including DAH.
-
DOACs - DOACs stands for ‘Direct Oral Anticoagulants’, and they can be categorised into these main classifications: oral direct factor Xa inhibitors (e.g. rivaroxaban and apixaban), and direct thrombin inhibitors (i.e. dabigatran).
DOACs are also anticoagulants, but differ in the way they work. Whilst there are many advantages to DOACs, such as not needing to monitor vitamin K food intake, they are also generally not recommended for APS patients, especially if you are triple positive or have had a DVT or similar before. Learn more about DOACs, how they work, and how they differ from warfarin in this post.
-
dRVVT (dilute Russell viper venom time) - This is one of the tests used to check for lupus anticoagulant. See the section on Snake Venom for more information.
Pin to Your Antiphospholipid Syndrome Health Resource Boards:
E is for Embolus & Enoxaparin
Embolus
An embolus can be a blood clot, or piece of plaque that acts like a clot. It is called an ‘embolism’ when it travels from one site of the body to another. Whilst they mostly occur in veins, embolisms can also block arteries, and are usually found in the legs or feet (MedLinePlus, 2022a).
There are many types of embolisms; besides blood clots, they can consist of fat, tumours and even air. Depending on where the embolism is at, symptoms can include: shortness of breath, hypoxemia (low oxygen levels), hypotension (low blood pressure), headaches, swelling, and more. These can eventually lead to severe complications such as arrhythmia (abnormal heart rhythm), heart failure, kidney failure, stroke and more (Cleveland Clinic, 2024b).
Thus, it is important for APS patients to be aware that clots can consist of more than just blood product, and that they can lodge in unwanted places within the body beyond the veins – learn where in this post.
Enoxaparin
Enoxaparin (brand names: Lovenox and Clexane) (Drugs .com, n.d.) is also known as “low molecular weight heparin” (LMWH), and is an anticoagulant with a much shorter half-life as compared to warfarin (Cook, 2010). It is commonly used as a bridge medication when an APS patient needs to stop taking warfarin temporarily. Common scenarios are surgeries, both major and minor, where bleeding might be anticipated, as well as during pregnancies.
Whilst enoxaparin is derived from heparin, it is important to note that the final formulation as well as administration differ (U.S. Food & Drug Administration [FDA], 2018).
Learn more about enoxaparin and heparin here.
Other Words Starting with ‘E’ for APS:
-
Etonogestrel (Implanon & Nexplanon) - As oestrogen is known to increase the risk of blood clots, birth controls containing this hormone generally need to be avoided if you have Antiphospholipid Syndrome (Rosendaal, 2003).
Etonogestrel is a progestin hormone that is sold under the brand names, Implanon and Nexplanon (Cleveland Clinic, n.d.; RxList Inc., 2022; Nexplanon, n.d.). It comes in the form of a small implant that is inserted subdermally in your arm by your gynaecologist. Learn more about birth control and women’s health in relation to APS here.
- Estrogen - See Oestrogen.
-
“Euro-Phospholipid” Project - The Euro-Phospholipid Project started in 1999, where 1000 Antiphospholipid Syndrome patients from 13 European countries have been followed since. It provides some interesting medical insights into APS, and correlations with other comorbidities such as Lupus (SLE). You can view the paper on the lessons gleaned from the Euro-Phospholipid Project here (Cervera, 2008). You can also read this post for the latest research insights into Antiphospholipid Syndrome.
Pin to Your Antiphospholipid Syndrome Diagnosis Boards:
F is for Free Fluid & False Negative/Positive
Free Fluid
Intra-abdominal fluid collections can be classified into: free intraperitoneal fluid and contained fluid collections (Mansoori & Herrmann, 2013). Free (intraperitoneal) fluid can build up quickly and cause severe pain. An ultrasound is usually used to detect free fluid in patients with acute pain in an emergency setting.
This was what happened to me twice when I experienced ovarian cyst ruptures that would not stop bleeding, due to being on warfarin. The pain escalated quickly in a mere 4 hours, from mild to a life-and-death situation. Learn more about ovarian cyst ruptures and menstruation in this post.
False Negative/Positive
A false negative is also known as a “type II error”, and is pretty self-explanatory (a negative result is obtained when it should actually be positive). A false positive (“type I error”), is the reverse, where a positive result is obtained, when truly it is negative (Exploring Our Fluid Earth, n.d.).
Whilst I’m not grateful to have Antiphospholipid Syndrome, I’m grateful that my initial diagnosis was straightforward. After suffering a transient ischemic attack (‘mild stroke’), they did a blood test and confirmed a diagnosis of APS.
Diagnosis isn’t always so straightforward however for a myriad of reasons. Patients can present with a wide range of symptoms that overlap with other health conditions or autoimmune diseases. False-positives can also occur as a result of certain medications of after having caught an infection, such as syphilis.
False-negative/seronegative APS patients are harder to diagnose and therefore treat, as they usually present with clinical symptoms, yet no antiphospholipid antibodies are detected in their blood (Lockshin et al., 2000). Understandably, this is extremely frustrating for both the patient and doctor.
Read the section on Non-Criteria/Seronegative APS for more information.
Other Terms for ‘F’ & APS are:
-
Factor V Leiden - This is another type of blood clotting disorder that also increases the tendency for abnormal blood clots to form. The difference is that Factor V Leiden is a hereditary disorder, where a mutation of one of the clotting factors increases the risk of blood clots (Ornstein & Cushman, 2003).
Whereas Antiphospholipid Syndrome is an autoimmune disease, where the body produces antibodies that attack tissues in the body and causes blood clots to form. There is a nice infographic on the differences here (Udayangani, 2022).
-
Factor Xa Inhibitors - These are another class of blood thinning medications, also known as direct oral anticoagulants (DOACs). In general, APS patients, especially those who are high risk, need to stick with warfarin instead. You can read more about DOACs, and why warfarin is recommended instead for APS patients here.
-
Fruits - You might be surprised, but it isn’t only the green foodstuffs that can interact with warfarin. According to Norwood et al. (2015):
“A total of 23 citations (15 case reports and 7 controlled clinical trials) were reviewed. The majority of cases involved cranberry products, while pomegranate juice, avocado, grapefruit juice, mango, and papain were also implicated in reports of suspected warfarin-fruit interactions.”
Mangoes have also been shown to increase the INR in 13 patients, who were consuming between 1 – 6 mangoes per day, for at least 2 days (yes, I am aware that nobody eats six mangoes a day, but that’s research for you 😆). Mangoes contain high levels of Vitamin A, which may inhibit CYP2C19, which is an enzyme that is involved in warfarin metabolisation (Norwood et al., 2015).
More research still needs to be conducted to determine the interaction between warfarin and fruits, but it never hurts to monitor your INR levels if you’re on warfarin, and consume any new food product. From there, you will slowly learn how to balance your diet in relation to your warfarin dosage.
Read this post for more information on warfarin interactions.
Pin to Your Antiphospholipid Syndrome Diagnosis & Medical Resource Boards:
G is for Genes & Green, Leafy Vegetables
Genes & APS
Genes are complicated things, aren’t they? As with any autoimmune disease, genetics have a complex interplay in Antiphospholipid Syndrome, where factors such as environment, trauma and comorbidities also need to be accounted for. In a warped sense, the body is pretty amazing in its ability to mess itself up.
According to Barinotti et al. (2020):
“The impact of a specific genetic alteration is not restricted to the activity of the gene product carrying it, but it can also alter products of genes that actually do not carry defects [83,84,85]. Thus, in order to better understand complex and multifactorial disorders, such as APS, and the consequences of genetic abnormalities, it is important to look at a gene as a part of a complex network of processes and interactions and not as an isolated entity.”
There have been various studies on familial risk factors in Antiphospholipid Syndrome, yet the results are inconclusive due to the heterogeneity of antigen specificities and clinical manifestations of APS patients. What is fairly certain is that a few genetic abnormalities and factors are probably needed to ‘click’, to set Antiphospholipid Syndrome and its consequences into motion (Castro‐Marrero et al., 2009).
Another interesting thing to note is that Antiphospholipid Syndrome isn’t passed down directly from parent to child like some other autoimmune diseases (NHS, 2022a). You can learn more about polygenes here.
Green, Leafy Vegetables
Green, leafy vegetables, as well as certain legumes and vegetable oils contain a fairly high amount of Vitamin K1. If you’ve just received an Antiphospholipid Syndrome diagnosis and are on warfarin, your doctor would highlight this to you as it’s important to remember.
Having said that, moderation is always key when it comes to warfarin management, as the dosage is adjusted to your regular diet (Jaffer & Bragg, 2003). I will cover APS and food in a separate post, as it’s a complex topic. In the meantime, you can read more about warfarin medication interactions here.
Other Words for ‘G’ & APS are:
-
Google Alerts - Not directly related to APS, but Google Alerts and RSS Feeds are a great way to stay on top of the latest news and research about it. Learn how to use them to keep up with the latest research on Antiphospholipid Syndrome here.
-
Green Tea - I’m not sure about other countries, but this was one of the first food and drink items that the doctor told me to avoid when I first received my Antiphospholipid Syndrome diagnosis. Green tea is a pretty potent coagulant, although it does have anti-inflammatory health benefits that may help with managing other autoimmune conditions such as Lupus (Mount Sinai, n.d.-a; Wang et al., 2014).
Green tea has also been reported to have an antiplatelet effect, which increases bleeding, so it seems to have multiple properties as well (Nutescu et al., 2006). This is a common conundrum for those with APS, as so many beneficial foods need to be moderated due to warfarin intake.
Pin to Your APS & Autoimmune Disease Boards:
H is for Hughes’ Syndrome, Herbs, Haemorrhage & Heparin-Induced Thrombocytopenia
Hughes’ Syndrome
Antiphospholipid is also known as Hughes’ Syndrome, after the doctor who first described it in 1983 (Hughes, 2007). (Fun fact: I’ve visited him in person in London!) I suppose “Hughes’ Syndrome” is easier to remember and pronounce as compared to “Antiphospholipid Syndrome”, though the latter does have a nice pitter-patter ring to it.
Herbs
Herbs are tricky things; there are so many superfoods and traditional herbs touted for their health benefits. They might even be beneficial in the management of other chronic illnesses, such as Lupus (SLE). Yet, there is little medical literature on the interaction between such herbs, and their blood thinning or blood clotting effects.
Having experimented with common Chinese and Indian herbs in soups and foods – sometimes unintentionally – I was surprised to find out how quickly my INR could swing. I didn’t have to consume a lot of these herbs for that to happen, and thus I approach them with great caution. I try to find information about the herb on Google, and only taste a little if it’s something I’ve never tried before. I then compare my INR the next day with my CoaguChek machine, to see what difference it made, if any.
According to Chua et al. (2015):
“This review has evaluated the current published evidence regarding the herb-warfarin interactions of 44 commonly used Chinese herbal products in Singapore. Of these, 11 herbs (danshen, ginkgo, dong quai, American ginseng, safflower, peach kernel, licorice, Asian ginseng, lycium, ginger and notoginseng) were found to have the strongest evidence of potential interaction with warfarin.”
I will be writing a separate post dedicated to herbal interactions with Antiphospholipid Syndrome, because it is a mega topic that could take up half the content on this page, so keep an eye out for it! Sign up for my newsletter here should you wish to be kept in the loop.
In the meantime, you can read more about warfarin medication interactions here.
Haemorrhage
This is the medical term for excessive bleeding. So why are we talking about bleeding, when Antiphospholipid Syndrome is a blood clotting disorder? This is because the medications used for the management of APS are mostly anticoagulants, which thin the blood and therefore, increases the risk for bleeding ironically.
I’ve suffered from a few of such haemorrhagic events, where different types of coagulants were used in an attempt to stop the bleeding. You can read about my experiences at the Emergency Department here, where another hospital refused to accept me for treatment due to the ‘high risk’.
This is also the reason why your INR needs to be monitored if you are on warfarin – to ensure that your blood is ‘thin’ enough, but not too much. Intravenous (IV) vitamin K is usually administered to reverse the effects of warfarin during a major haemorrhagic event (Hanley, 2004). Learn more about reversal agents and the reversal protocol here.
Heparin-Induced Thrombocytopenia (HIT)
Heparin-Induced Thrombocytopenia (HIT) is a severe complication that occurs from the use of any products containing the drug, heparin. The main symptoms are a fall in platelet count and a hypercoagulable state, which can be life-threatening (Nicolas et al., 2023).
There are two types of HIT – Type I HIT and Type II HIT – with the latter being more severe as it is activated by antibodies. According to Nagano et al. (2023), currently the thrombin inhibitors used for HIT therapy do not have antidotes, although they are working on one. There is also some interesting research into a new drug to combat HIT. You can also learn more about heparin here.
Other Important Terms Under ‘H’ for APS are:
-
Haemophilia - You’ve probably heard of Haemophilia, also known as the ‘Royal Disease’ that affected English, German, Russian, and Spanish nobility. So I guess it has more awareness due to such publicity (Hickey, 2023).
Haemophilia is kind of (and not) the opposite of Antiphospholipid Syndrome. Both are blood disorders; in APS, the blood tends to clot, whereas in Haemophilia it does not clot properly, which leads to bleeding. APS is also more common in females (approx. 70%), whereas Haemophilia in males (for both Haemophilia A and Haemophilia B) (MedLinePlus, 2022b; National Bleeding Disorders Foundation [NBDF], n.d.-a; NBDF, n.d.-b).
Haemophilia is also an inherited disorder, whereas multiple genetic and environmental factors play a role in APS, with no clear pattern of inheritance (Centers for Disease Control and Prevention [CDC], 2024b; MedLinePlus, 2022b).
-
Heart Attacks - Read this post for more information on cardiovascular disease and Antiphospholipid Syndrome.
-
Heparin - Heparin is given intravenously only within a hospital setting. It has a higher chance of causing Heparin Induced Thrombocytopenia (HIT), where massive activation of platelets take place, with multi-cellular release of micro particles that contribute to hypercoagulability in patients (Gruel et al., 2020). Hence, patients need to be closely monitored. Learn more about heparin and other APS medications here.
-
Hospital Bag - If you’ve been chronically ill for a while, chances are you have a ‘go bag’ for emergency trips to the hospital. I have one packed with a few days’ supply of medications, a change of clothing, underwear, hygiene products, a powerbank, water bottles, slippers, and other basic supplies I may need at the A&E, or should I need to be admitted. It can be a hassle to write down a list of things for your family members to bring, and they may not be able to find everything you need either.
Pin & Help to Share This Antiphospholipid Syndrome A to Z Guide:
I is for INR, Infections & Injections
INR (International Normalised Ratio)
A “PT” (Prothrombin Time)/INR blood test must be done regularly for all Antiphospholipid Syndrome patients who are on warfarin. The PT/INR blood test measures how quickly it takes for your blood to clot, so that your doctor can adjust your warfarin medication accordingly, if needed. PT tests can also be used to check for blood clotting and bleeding conditions, and how well your liver is working (Healthdirect Australia, 2022).
Infections: Both the Trigger & Target
Infections can either be the trigger to Antiphospholipid Syndrome, and/or worsen clinical manifestations in APS patients. According to Radic and Pattanaik (2018), certain infectious agents might interact with β2GPI, which has implications in Antiphospholipid Syndrome. Other possible mechanisms for activation of disease include molecular mimicry, as well as an abnormality in immune-related protein and blood components.
According to Shoenfeld et al. (2006), many infections are often accompanied by an increase in aPLs (antiphospholipid antibodies). Some of these infections include, but are not limited to: skin infections, human immunodeficiency virus (HIV) infection, Hepatitis C (Hep C) virus, urinary tract infections (UTIs) and more (also see: Cervera et al., 2004). The two most commonly reported viral infections associated with aPLs are HIV and Hep C (Martirosyan et al., 2019).
Shoenfeld et al. (2006) also propose a two hit hypothesis; in the first hit, aPLs increase the risk for thrombosis, and in the second hit, involvement of TLRs (toll-like receptors) by microbial structures together with those mediated by anti-β2GPI antibodies have a synergistic effect that contribute to the clotting event.
According to a review by Mendoza-Pinto et al. (2018), all types of infections can trigger APS, from bacterial to parasitic and fungal, but especially viral. Certain vaccines can also trigger APS. One thing to note is that the existence of aPLs are mostly transient for an otherwise healthy person who has caught an infection; that is, the levels may rise in the patient’s blood for a period of time, but usually subside without further incidence (also see: Martirosyan et al., 2019).
You can learn more about which major organs APS can hit in this post.
Injections as an APS Patient
In general, subcutaneous injections are okay for people who are on anticoagulants, as they penetrate into the fatty tissue just beneath the skin (MedLinePlus, 2023). This is also how people with Antiphospholipid Syndrome self-administer enoxaparin (Clexane/Lovenox) as well. You can learn more about enoxaparin here.
Intramuscular injections are a little trickier, as there is a risk of bleeding and muscle haematomas (Australian Immunisation Handbook, 2023). Patients who are on blood thinners generally need to stop taking them before receiving an intramuscular injection or vaccine (such as the HPV vaccine (CDC, 2021). Learn more about the reversal protocol here.
In some cases, such as an epinephrine injection during an anaphylaxis reaction, it cannot be avoided. In such cases, the patient should be monitored until healthcare professionals have deemed that both bleeding and clotting risks are well under control. This was what happened to me when I was undergoing rituximab treatment for Lupus at the hospital, and suffered an allergic reaction to it.
Other Terms for “I” and APS:
-
Immunosuppressants - There are some immunosuppressants, such as azathioprine, and many other medications that interact with warfarin (Ng & Crowther, 2006; UpToDate, n.d.). You will need to work with your doctor(s), if you need to take a medication for a comorbidity that interacts with warfarin.
Your warfarin dose will most likely need to be tweaked, to ensure that your INR is within your personal target range. Always consult your own doctor before changing or taking medications that might potentially interact with warfarin. Learn more about warfarin drug interactions here.
-
Implanon - This is the brand name of a birth control implant that contains etonogestrel, a progestin-based hormone. Read more about Implanon, hormones and birth control here.
-
Inflammation - Antiphospholipid Syndrome is a thrombo-inflammatory autoimmune disease, with ongoing research as to its role within the immune system. Inflammation can be activated from various pathways, with antiphospholipid antibodies as a contributing factor (Ambati et al., 2023). You can also learn more in this post on the systemic implications of Antiphospholipid Syndrome.
-
Interactions - There are many everyday activities that can interact with warfarin and Antiphospholipid Syndrome, such as your diet and contact sports. APS patients need to be careful of getting hit (even ‘gently’ at times!), as they can bruise and bleed easily.
I use MedScape (n.d.) all the time to check for medication interactions with warfarin and also other drugs. Another alternative medication interaction checker is DrugBank (n.d.). I have the MedScape app downloaded on my iPhone, and you can also get it at the Google Play app store. Learn how it works and how I use the MedScape app here.
-
Invisible Illness - Antiphospholipid Syndrome is dangerous because it is an invisible illness. In fact, it may not present with any pain symptoms, but when it strikes, it goes in for the kill. This was my fatal mistake as a teenager.
I presumed that I was fine since I did not experience any pain, and continued to eat, drink and play sports as per usual. That was until I developed multiple DVTs and a pulmonary embolism that nearly costed me my life. The event also activated all my other autoimmune diseases and chronic illnesses subsequently. So learn from my mistakes and pay attention to your body, whether you feel any pain at present or not.
Read more about how Antiphospholipid Syndrome can affect your entire body in this post.
Pin to Your Antiphospholipid Syndrome Diagnosis Boards:
J is for Juicing
You know how they tell you that kale (or whatever vegetable) juice is going to work miracles for you? Well, you might want to avoid that with Antiphospholipid Syndrome, as green leafy vegetables tend to contain high levels of vitamin K, which is a coagulant and interacts with warfarin.
Having said that, consistency is key. According to Booth and Centurelli (1999) (they have a comprehensive list of common foods that contain vitamin K, too):
“When a dietary vitamin K interaction with warfarin is suspected, inconsistent consumption of green vegetables is often the cause of fluctuations in vitamin K status.”
So if it is part of your daily routine to drink a cup of kale juice every single morning, then you need to stick to it every day. Warfarin dosages are adjusted based on your personal diet and not someone else’s. This is why warfarin management can be tricky, especially when you first receive an Antiphospholipid Syndrome diagnosis, as it’s difficult to know where to even begin diet-wise.
Should you wish to add or remove something that interacts with warfarin from your daily or weekly diet plan, then you need to discuss this with your doctor. They will monitor your INR closely, and should work with you to make that shift happen. Learn more about warfarin and its interactions here.
Pin to Your Antiphospholipid Syndrome & Healthy Living Boards:

K is for Vitamin K
Vitamin K is the vitamin that patients with an Antiphospholipid Syndrome diagnosis become most familiar with eventually, as it interacts with warfarin and contributes to the blood clotting process (Office of Dietary Supplements [ODS], 2021). It’s a little ironic because most people are more familiar with vitamin C and vitamin E, but don’t fully understand what vitamin K does. Neither do they know which foods and drinks contain it.
Apart from blood coagulation, vitamin K is also important for many other bodily processes. It works together with vitamin D to promote bone health, prevent vascular calcification and also modulate cell proliferation (Bus & Szterk, 2021). There has also been recent interest in vitamin K’s role in intestinal health (Lai et al., 2022). Thus, whilst it is important to monitor your vitamin K intake, it is also important to take into account your body’s overall nutritional needs.
Types of Vitamin K
Vitamin K is not quite a vitamin, but a family of compounds that share a similar chemical structure, 2-methyl-1,4-napthoquinone. These are primarily vitamin K1 (phylloquinone) and vitamin K2 (a series of menaquinones). A synthetic version exists as well in the form of vitamin K3 (menadione), although it is no longer used in food products due to evidence that it can damage hepatic cells (ODS, 2021).
According to Booth (2012), all photosynthetic plants produce vitamin K1, with green, leafy vegetables containing the highest concentration. Vitamin K2 is primarily of bacterial origin and can be found in food products such as fermented foods. MK-4 (menaquinone-4) is the exception, as it is mostly found in dairy products, and also as a result of vitamin K1 or K3 conversion within the body.
Vitamin K is Heavily Diet Dependent
No matter what form it comes in, vitamin K is fat-soluble, although the bioavailability, absorption and storage varies. Humans also do not produce vitamin K, and need to rely on dietary intake to meet the body’s requirements for it (Simes et al., 2020). In addition, the human body recycles vitamin K as only a minute amount of it is retained (Fusaro et al., 2017).
As vitamin K intake is heavily dependent on diet which varies by country and person, it has been hard to pin down a fixed daily intake requirement even up to this day (Booth, 2012). In most Western nations, the main form of vitamin K intake is vitamin K1, whilst in Japan, it is vitamin K2 (Fusaro et al., 2017).
I will be writing a separate post that focuses on vitamin K, as I realised this section would become too lengthy if I kept adding to it 😉 You can learn more about warfarin and medication interactions here.
Pin to Your Vitamins, Nutrition & Antiphospholipid Syndrome Boards:
L is for Lupus & Lupus Anticoagulant
Lupus Anticoagulant – A Double Misnomer
It’s important to note that there is a difference between Systemic Lupus Erythematosus (SLE / the autoimmune disease) (CDC, n.d.), and the lupus anticoagulant (a heterogeneous class of immunoglobulins).
The ‘anti’ in ‘lupus anticoagulant’ is actually a misnomer with historical roots, as it was originally found to prolong a clotting test that is dependant on phospholipids in Lupus patients. Later, it was discovered that the lupus anticoagulant actually increases the tendency for the blood to clot (Wong et al., 1987).
The ‘lupus’ in ‘lupus anticoagulant’ is also a misnomer, as more than half of people who have this antibody do not indeed have Lupus (the autoimmune disease). So you can see how Lupus and lupus anticoagulant are easily confused!
Lupus (SLE) & APS Overlaps
Having said that, it is also not unusual for patients with Lupus to be diagnosed with APS, and vice versa. Both autoimmune diseases are closely linked, with a spectrum of overlaps in clinical manifestations. For some patients, it is considered Primary APS with Secondary Lupus, or the other way around, depending on their manifestations (Radic & Pattanaik, 2018).
SLE occurs more frequently in females than in males with a 9:1 ratio, and generally manifests during the fertile period between 15 – 50 years of age. The clinical manifestations may differ a little between female and male patients. Antiphospholipid antibodies are also frequently found in SLE patients (at least 20-30%) (Pons-Estel et al., 2017).
Testing for Lupus Anticoagulant (LA)
The lupus anticoagulant (LA) is one of several criteria used to diagnose Antiphospholipid Syndrome. Not all APS or Lupus patients will test positive for the lupus anticoagulant, and detection of LA also consists of a sequence of tests, instead of just a single one (Pengo et al., 2009).
According to Rasool and Tiwari (2023), this sequence of tests for lupus anticoagulant include an initial screening test, a mixing study, and a final confirmatory test. You may be familiar with some of the tests used in this sequence, such as PTT and dRVVT. Rasool and Tiwari (2023) have also summarised the LA testing criteria as outlined by the International Society of Thrombosis and Hemostasis (ISTH) here:
- “(Screening test) Prolonged result in one of two coagulation tests that are phospholipids dependent such as PTT-LA or DRVVT
- (Mixing study) observe the prolonged result on mixing study
- (Confirmatory test) Lack of prolonged time when adding additional phospholipids
- Ruling out other coexisting coagulation factor inhibitor such as factor VII.”
The full guide on lupus anticoagulant testing can be found in the Journal of Thrombosis and Haemostasis, should you be interested to learn more (Devreese et al., 2020).
Lupus Anticoagulant – aPL Associated with the Highest Risk for Thrombosis
Of all the antibodies that mark Antiphospholipid Syndrome, patients with the lupus anticoagulant are also at the highest risk of thrombosis (Pengo et al., 2007). The odds ratio for thrombosis are 5 – 6 times higher, and presence of LA are both strong indicators for thrombosis and Systemic Lupus Erythematosus (SLE) (Galli et al., 2003). Hence, both APS and SLE patients need to monitor their LA markers periodically.
Another interesting thing to note is that patients who are on DOACs (except perhaps for apixaban) may yield false-positive results for lupus antibody (Hoxha et al., 2017). Clinical research is still ongoing for this. You can read about the latest APS research in this post, and also learn more about DOACs here.
Other Terms for “L” and APS are:
-
Labels - It’s important to check food labels when you first receive an Antiphospholipid Syndrome diagnosis, and are unfamiliar with what to eat. Food labels and percentages can give clues as to whether an ingredient might interact with your APS medications.
A little trick or tip is to avoid products that are labelled as ‘good for heart health’ or ‘not for pregnant women’, especially in supplement form. These consumable products generally have blood thinning effects, and supplements often come in a concentrated form. I will write a post on little APS hacks in future, when I can! In the meantime, you can learn more about warfarin interactions here.
Pin to Your Antiphospholipid Syndrome & Lupus Boards:
M is for Miscarriage, Men with APS & Musculoskeletal Manifestations
Miscarriages & APS
Recurrent miscarriages are a common indication of Antiphospholipid Syndrome (Di Prima et al., 2011). Apart from miscarriages, pregnancy with APS also comes with added risks. As this is an extensive topic, I have separated it into a post of its own. Read more about miscarriage, pregnancy and women’s health with APS here.
Antiphospholipid Syndrome in Men
Antiphospholipid Syndrome occurs more commonly in women than in men, with a ratio of about 3.5:1, but few studies have been done on how the disease manifests between sexes. Albeit the small sample sizes, here is what has been found so far in terms of prevalent APS manifestations between males and females (Truglia et al., 2022; Jara et al., 2005; Cervera et al., 2002):
Females: central nervous system, stroke / TIA (transient ischemic attack), pulmonary embolism and venous thrombosis at a young age.
Males: mesenteric thrombosis, Budd-Chiari syndrome, gastrointestinal complications, arterial thrombotic events (such as myocardial infarctions and peripheral thrombosis of lower limbs), later-onset but more relapsing arterial events and epilepsy.
Other research that has been found so far, albeit limited, is that males tend to have Primary APS more than Secondary APS, unlike women where the ratios found were closer in number. Female also tend to have more IgM anticardiolipin antibodies than males (Truglia et al., 2022; de Carvalho, 2011).
Musculoskeletal Manifestations
Several musculoskeletal manifestations have been reported in APS patients, namely: Arthralgia/Arthritis, Avascular Necrosis/Osteonecrosis, bone marrow necrosis, complex regional pain syndrome type-1 (reflex sympathetic dystrophy), muscle infarction, non-traumatic fractures and osteoporosis (Noureldine et al., 2016). Musculoskeletal manifestations can also be further complicated with comorbidities, such as Lupus (SLE). Learn more about musculoskeletal manifestations in APS patients here.
Other Terms for “M” and APS are:
-
Massages - Massage involves touch, and with that, a possibility of bruising due to the pressure applied. As a person with APS, I’m sure you’re familiar with how easily a bruise can form! Whilst I suppose that the safest solution to avoid blood clots is to not have any massages at all, I find life sad without them. Massages are very therapeutic for me, especially when I’m in a Lupus or Sjögren’s pain flare, and am aching everywhere. They truly do help me to sleep better at night, and ease some of the pain.
So what I do is to be stringent with the selection of a massage therapist, and also voice out when I think they need to reduce the pressure. I actually found a masseuse whom I really like, and I return to her all the time because she knows my body pretty well by now. I never get a bruise after her massages, and always feel much brighter and better after. Please note that I am simply sharing my experiences; do check with your own doctor if you would like to try massages as a pain management strategy for your other chronic illnesses.
-
Medical ID - When I was first diagnosed with Antiphospholipid Syndrome, I was given a medical card that stated I was on warfarin. I was told to keep this card close to me at all times, in case of an emergency. I also have other medical cards in my wallet that state I have antibodies in my blood, and that I have an annuloplasty band for a mitral valve repair. These are all important medical information, especially if you need a blood transfusion or emergency surgery done.
There is a risk of bleeding with surgeries, so my warfarin medication needs to be reversed. Having antibodies in the blood also means that they might need to filter blood from the blood bank for me, if they are unable to find an exact match (regardless of blood type). (Learn more about the reversal protocol for various anticoagulants here.)
Whilst first responders should always check for such medical information that a person may be carrying, this might not always be the case during a frantic emergency situation. Thus, some people wear medical IDs in the form of accessories such as bracelets or necklaces. This can help to alert paramedics and hospital staff that the patient has a medical condition they need to take note of, such as Antiphospholipid Syndrome.
-
Menopause - Whilst there are not many studies done on APS in relation to menopause, it is a period of immune changes within the body, one of which is a decrease in oestrogen (Bove, 2013).
-
Menstruation - Women with Antiphospholipid Syndrome can have heavier periods or see blood clots whilst menstruating (APS Support UK, n.d.). It is also important to be aware of ovarian cyst ruptures, as these are extremely painful and can be life-threatening. I’ve had the misfortune of experiencing them twice, and am now on a progestin-based birth control as a preventive method. Learn more about menopause, menstruation, birth control and ovarian cyst ruptures in this post.
-
Mental Health - Read this post for more information on neuropsychiatric symptoms in APS.
-
Movement - It’s important to keep on your toes when you live with a blood clotting disorder like Antiphospholipid Syndrome! This is especially true if you’re taking a long flight, due to the change in cabin pressure, dehydration, and cramped spaces. Even healthy people can get DVTs on flights, so it is even more vital for a person with APS to keep moving every hour. You can read more travel tips in my post here, and learn more about flights and DVTs in this post.
-
Magnetic Resonance Imaging (MRI) - An MRI procedure is the one where they slide you into a tube-like casing, then start to blare a sequence of loud, weird sounds at you (Mayo Clinic, 2023c). Unlike CT scans or x-rays, they do not use radiation but powerful magnets, so if you have metallic implants, do let the technician know. They produce three-dimensional images of anatomy in greater detail than x-rays or CT scans.
MRIs are most frequently used to diagnose brain and spinal cord issues, but can also be used to check on heart or blood vessels, bones and joints, as well as irregularities in other organs such as the kidney, uterus and prostate.
In particular, spin echo (SE) imaging is effective for intracardiac masses, such as thrombi and tumours. MRIs are also able to differentiate tumours and age of blood clots more clearly than echocardiograms. These insights can be useful for the formulation of treatment plans (Erkan et al., 2002).
It is also interesting to note that MRI findings of certain APS patients are similar to those with Multiple Sclerosis (MS). Whilst further studies need to be done, Stosic et al. (2010) conclude in a small MRI study that:
“The release of phospholipid antigenic determinants during tissue injury may play an important role in the epitope spreading of immune response and the generation of APLAs in MS that may lead to secondary ischemic damage.”
-
‘Muscular Sprains’ - Muscular sprains are something to be aware of, especially around your chest area, as they might indicate a Pulmonary Embolism (PE). As someone who has experienced the full works of haemorrhages, blood clots, tendon ruptures and muscle sprains, I can usually tell which is what by now.
For someone who is newly diagnosed with APS, it can be difficult to differentiate between a regular muscular sprain and a blood clot. I am here to tell you to please simply err on the side of caution, and visit your specialist or the ED/A&E right away.
When I experienced a PE at 17, I had initially visited a General Practitioner (GP) who brushed it off as a muscular sprain. I only went to the A&E two days later and by then, it was a little too late. This major health crisis triggered a cascade of autoimmune disorders that might have stayed dormant otherwise. Read more about pulmonary embolisms and other manifestations of APS here.
Pin to Your Antiphospholipid Syndrome Diagnosis & Resource Guide Boards:
N is for NSAIDs, Neuropsychiatric Manifestations & Non-Criteria APS
NSAIDs
Does “Ibuprofen”, “Naproxen” or “Aspirin” ring a bell? These all fall under a class of medications called NSAIDS (Non-Steroidal Anti-Inflammatory Drugs) (Harvard Medical School, 2019b).
In brief, NSAIDs interfere with the blood clotting process through the inhibition of platelet function. They also increase the risk for gastrointestinal bleeding and peptic ulcers due to the way they are metabolised (Drini, 2017). Thus, taking NSAIDs can pose as an additional risk when you are already on an anticoagulant drug. Learn more about NSAIDs here.
Neuropsychiatric Manifestations
Neuropsychiatry is a field of medicine that involves both neurology and mental illness (Royal College of Psychiatrists, n.d.). Whilst a lot more research still needs to be done, Antiphospholipid Syndrome is now recognised as a major neurological disease as well. Neurological events include: strokes, TIAs, migraine, headaches, brain fog/cognitive dysfunction and much more (Hughes, 2003).
I write about neuropsychiatric manifestations in APS patients more comprehensively here.
Non-Criteria APS / Seronegative APS
This is a widely debated topic amongst researchers and even amongst patients. In basic terms, non-criteria APS (NC-APS) indicates that a person may have Antiphospholipid Syndrome, but does not meet the formal criteria for it (see the section on Antiphospholipid Syndrome for what those are). Non-criteria APS patients can present with clinical manifestations such as strokes, migraine, livedo reticularis, thrombocytopenia and others, yet blood tests yield a negative result for apLs (Pires da Rosa et al., 2020).
Cervera et al. (2012) makes a case for and against testing for so-called non-criteria APS antibodies, and concludes with a rough protocol to follow in terms of diagnosis. For instance, serum IgG anti-vimentin/cardiolipin antibodies can be found in a large number of NC-APS patients, and in almost all patients who have a confirmed APS diagnosis. However, antiphospholipid antibodies (aPLs) can also be transient in nature. These are just two examples from Cervera et al.’s (2012) paper for and against testing for NC-APS.
Read this post for all the various manifestations that Antiphospholipid Syndrome can present as.
Types of Non-Criteria APS Antibodies
Liu et al. (2022) investigates seven of these non-criteria antiphospholipid antibodies, which include:
- anti-phosphatidylserine/prothrombin (aPS/PT) antibodies IgG/IgA/IgM,
- anti-phosphatidylethanolamine antibodies (aPE) IgG/IgA/IgM,
- anti-Annexin V antibodies (aAnnexinV) IgG/IgA/IgM,
- anti-phosphatidylserine antibodies (aPS) IgM,
- aPS IgG,
- antibodies directed against a mixture of phospholipids (APhL) IgG, and
- APhL IgM
They conclude that the highest prevalence of non-criteria aPLs was aAnnexinV, whilst APhL IgG and aPS IgM had the highest specificity, and aPS/PT had the highest Youden index for diagnostic value in terms of APS. Of these seven non-criteria aPLs, they further conclude that three in particular – APhL IgG, aPS/PT, and aPS IgG – might show potential as biomarkers for APS-related thrombosis events.
Classifications for ‘Seronegative’ & ‘Non-Criteria’ APS
In a small study of seronegative APS patients, Truglia et al. (2022) found that 69% of them tested positive for at least one non-criteria test. Interestingly, seronegative APS patients who tested positive for aVim/CL IgA showed a higher prevalence of arterial thrombosis, whilst APS patients who tested positive for aVim/CL IgG showed a higher prevalence of pregnancy morbidity and thrombocytopenia (Capozzi et al., 2021).
To complicate matters, definitions and terms can vary from paper to paper, and different laboratories may produce different results. According to Cervera et al. (2012), even anti-β2GPI, which is a known antiphospholipid antibody, is only tested in a small number of labs. Much of the literature for non-criteria APS also focuses on obstetric patients, where majority seem to be treated as ‘regular’ APS patients, despite being seronegative (Pires da Rosa et al., 2020).
As a result, Pires da Rosa et al. (2020) further proposes breaking down non-criteria APS into the following four categories: “Seronegative APS”, “Clinical non-criteria APS”, “Incomplete laboratory APS” and “Laboratory non-criteria APS”. This might help to break this quandary down into more identifiable parts for further research.
Other Terms for “N” and APS are:
-
Nexplanon – Read more about Nexplanon and birth control here.
-
NOACs (novel oral anticoagulants) - This is another name for DOACs, and is also the name that has been used for the longest amount of time. However, for the purpose of clarity, the term “DOAC” is preferred (Barnes et al., 2015). Learn more about DOACs in this post.
-
Numbness - Numbness, or a “pins and needles” sensation, can be a sign of poor blood circulation, or one of many symptoms of a blood clot. Please seek medical attention immediately if you think you might have a blood clot, as the consequences can be deadly. For example, half of my entire body went limp and numb when I experienced a Transient Ischaemic Attack (“mild stroke”).
Pin to Your Antiphospholipid Syndrome Diagnosis Boards:
O is for Oestrogen, Ovarian Cyst Ruptures & Ophthalmologic Manifestations
Oestrogen
Oestrogen (or estrogen) is a steroid hormone associated with menstruation that can increase the risk of both arterial and venous thrombosis (Delgado & Lopez-Ojeda, 2023). These are often used in contraceptives or as postmenopausal hormone replacement therapy (Rosendaal et al., 2002). If you have APS, it is important to use alternative therapies such as contraceptives that are progestin-based instead.
Ovarian Cyst Rupture
Ovarian cyst ruptures happen when a corpus luteum cyst occurs after the egg is released, and the opening becomes blocked in the corpus luteum (Mayo Clinic, 2023b). For women with APS who are on anticoagulants, this can result in internal bleeding and is a medical emergency. I nearly died from these ovarian cyst ruptures, which you can read all about here.
Learn more about oestrogen and ovarian cyst ruptures in this post.
Ophthalmologic / Ocular Manifestations
Ophthalmology is a field in medicine with many sub-specialties, and deals with the eyes and vision, their functions and diseases (Churchill & Gudgel, 2024). It is important to be aware that there are a number of ocular and neuroophthalmic manifestations that can happen in APS patients, including but not limited to: retinal arteritis, retinal venous occlusion, ischemic optic neuropathy, transient loss of vision, and diplopia (Suvajac et al., 2007).
You can learn more about ocular manifestations in Antiphospholipid Syndrome here.
Other Terms for “O” and APS are:
-
Osteopenia & Osteoporosis - Osteopenia refers to bone density loss, whilst osteoporosis to weak, brittle bones. Both are linked to bone mineral density, which is measured by a bone density test (Harvard Medical School, 2021b). Long-term warfarin use has been found to be a major contributor to osteoporosis (Yokoyama et al., 2020). Learn more about osteopenia, osteoporosis, and other musculoskeletal manifestations in APS patients here.
-
Omega Oils - Omega oils come in omega-3, 6 and 9. Omega-3 fatty acids are healthy fats that cells in the body require for proper functioning (Adili et al. 2018). They are also anti-inflammatory, and are beneficial for cardiovascular and neurological health. They come in three forms, which can be found in seafood such as fatty fish (e.g. salmon and mackerel), and plants (e.g. flaxseed and chia seeds).
Omega-6 fats are mainly found in vegetables, and also help to lower cholesterol when balanced with omega-3. Good sources of omega-6 polyunsaturated fats include: sunflower oil, soybean oil and evening primrose oil (Harvard Medical School, 2019a). Omega-9 fatty acids can be found in plant food sources such as macadamia nuts, soybean oil, olive oil and sunflower oil. They also bear anti-inflammatory and anti-cancer properties (Farag & Gad, 2022).
Whilst generally safe for the average person, certain omega-3 and omega-6 fatty acids have also been shown to have antiplatelet effects, which can prolong bleeding time especially for patients who are on anticoagulants (DiNicolantonio & OKeefe, 2019).
According to Adili et al. (2018):
“[omega]-3 and [omega]-6 polyunsaturated fatty acids are an essential component of the platelet phospholipid membrane and play a major role in regulation of platelet function. Dietary supplementation with [omega]-3 or [omega]-6 PUFAs may alter platelet lipid membrane phospholipid composition and affect platelet function, which, in turn, may alter the progression and thrombotic complications of cardiovascular disease.”
As such, it is better to get your nutrition from omega oils via natural food sources, as fish oil capsules and the likes tend to have a higher potency. Should you insist on or need such supplements, do discuss with your doctor so that they can adjust your medications accordingly.
Pin to Your Antiphospholipid Syndrome Diagnosis Boards:
P is for Pulmonary Embolism, Pregnancy, Phospholipids & Primary Antiphospholipid Syndrome
Pulmonary Embolism (PE)
A pulmonary embolism (PE) is when a blood clot travels to lodge itself in your lung, thereby restricting blood flow (Cleveland Clinic, 2024a). When I had a pulmonary embolism at 17, I experienced difficulty breathing and could not lie down flat. The GP I had seen had carelessly misdiagnosed it as a muscular cramp, so I waited for two days before rushing to the A&E – barely alive.
A pulmonary embolism is a medical emergency, so if you are experiencing chest pains that will not recede, please just err on the side of caution and visit the A&E/ED. Learn more about pulmonary embolisms here.
Pregnancy in APS Patients
Pregnancy with Antiphospholipid Syndrome is a topic that needs its own article; I cover pregnancy with APS in detail in this post. For a quick overview, this paper by Schreiber and Hunt (2019) does an excellent job of listing out the management of APS in pregnancy.
Phospholipids
Phospholipids are a class of lipids (fatty compounds) that are part of all major tissues in the body, and are concentrated in organs that require neuronal (nerve) interactions (Pichot et al., 2013).
According to Rege and Mackworth-Young (2015):
“Phospholipids are the major component of cell membranes. These molecules constitute approximately 60% of the dry weight of the brain and play an important role in neurodevelopment.” ….. “Phospholipids also facilitate signal transduction responses to neurotransmitters, such as serotonin, dopamine, glutamate, and acetylcholine that play a key role in the pathophysiology of psychiatric disorders.”
In basic terms, people with APS produce antiphospholipid antibodies (aPLs) that attack phospholipids, which leads to blood clotting issues. Phospholipids are also major components of cell membranes, including those in the brain. This means that beyond the blood, Antiphospholipid Syndrome can also lead to systemic issues, which I expand on in this post.
Primary Antiphospholipid Syndrome (PAPS)
Primary Antiphospholipid Syndrome (PAPS) is a term that mainly refers to patients who only have APS as an autoimmune disease, although it can morph to secondary APS (SAPS) further down the road. There are some clinical differences between PAPS and SAPS patients, such as valve lesions, which occur more frequently in PAPS patients (Asherson & Cervera, 1994).
In a small study of 60 Egyptian patients, it was found that PAPS patients were more likely to have cutaneous manifestations, and also higher levels of β2 glycoprotein I IgG, as compared to SAPS patients (Morad et al., 2022). In another European study of 1000 patients, the results showed that SAPS patients were more prone to arthritis, livedo reticularis, thrombocytopenia and leukopenia (Cervera et al., 2002).
What is key to keep in mind with an Antiphospholipid Syndrome diagnosis however, is that we can experience any symptom regardless of whether it is primary or secondary. So don’t hesitate to seek professional advice and care should you feel that something is not quite right. As my rheumatologist has mentioned to me – I may have secondary APS, yet my clinical manifestations thus far has been worse than even triple positive patients.
Read this post to learn more about how Antiphospholipid Syndrome can affect the entire body, from the blood to skin, eyes, lungs, brain, heart and much more.
Other Terms for “P” and APS are:
-
Paediatric APS - If APS is rare, then paediatric APS is even rarer. Not much is known about it, and there are no validated guidelines or criteria to help manage it better as of yet.
According to Basaran et al. (2020), children with APS tend to have more blood clots in the brain and ischaemic strokes, as compared to adults. Children with APS are also more likely to have a Lupus comorbidity, and the frequency of occurrence is similar in girls and boys. Acquired risk factors in adults are also generally not applicable in children (e.g. atherosclerosis, use of oral contraceptives, smoking, etc), and thus test results might differ.
In the 15th International Congress on Antiphospholipid Antibodies Task Force on Pediatric Antiphospholipid Syndrome Report (Soybilgic et al., 2017), they also note that platelets in infants have decreased function, and whilst certain coagulation proteins reach adult levels by age 5, in newborns this is different qualitatively. Paediatric strokes are also extremely rare, but can happen to children with APS (Marzooq, 2023).
-
Painkillers - There are a few different classes of painkillers, such as paracetamol/acetaminophen, NSAIDs, opioids and local anesthetics. Some antidepressants and antiepileptics are also used to manage certain types of pains (Queremel Milani & Davis, 2023).
If you have an Antiphospholipid Syndrome diagnosis, it is important to note that NSAIDs (e.g. ibuprofen, naproxen, aspirin, etc) not only interact with warfarin, but can also cause gastrointestinal bleeding and ulcers (Drini, 2017).
Thus, I only take NSAIDs when I have a high fever – but not before letting my healthcare team know beforehand. I also developed an allergy to paracetamol after having taken it too often during my pulmonary embolism episode, and am only left with opioids for managing my Lupus and Sjögren disease pain flares. Learn more about NSAIDs and Antiphospholipid Syndrome here.
-
Paper Cuts! - Yes, I had to include this one. I once had a paper cut whilst travelling overseas, and it wouldn’t stop bleeding for hours. So I bandaged it up real tight, and woke up the next day to a blue, numb thumb. I panicked and thought that I might need to get it amputated, because I could no longer feel it at all. Thankfully it settled down, blues, cuts and all.
P.s. Don’t forget to bring a bottle of ‘Stop Bleed’ spray or plasters, for situations like these whilst travelling! You can also check out my top tips for travelling with chronic illness and disability in this post.
-
Periods – Read more about menstruation and Antiphospholipid Syndrome here.
-
Platelets - Platelets are also known as thrombocytes, and are made in the bone marrow. They make up part of our blood, and play an important role in the coagulation process. Certain conditions can contribute to a low platelet count, such as thrombocytopenia and chemotherapy. Apart from donating blood, you can also donate platelets, which many patients need in order to survive (American National Red Cross, n.d.). (Learn more about thrombocytopenia here.)
According to Baroni et al. (2017):
“Although underestimated, platelets may be involved in APS and its thrombotic manifestations, especially arterial, in several ways. Thrombocytopenia is the most relevant non-criteria manifestation of APS, possibly caused by direct binding of anti-β2-GPI antibodies or anti-β2-GPI–β2-GPI complexes.”
Meaning to say that anti-beta2-glycoprotein 1, an antiphospholipid antibody, directly interacts with platelets. According to Huang et al. (2021), this increased risk for arterial thrombosis is due to upregulation of plasma levels of active VWF (Von Willebrand Factor), which promotes platelet activation. The lupus anticoagulant (LA) was also found to have the strongest effect on arterial thrombosis.
Other pathways and cell types have also been linked to platelet activation and Antiphospholipid Syndrome. On top of that, platelet dysfunctions may also contribute to antiphospholipid antibodies (Tohidi-Esfahani et al., 2024).
-
Point-of-Care Testing - Point-of-care (POC) testing simply refers to a medical test that isn’t done in a laboratory. You might be familiar with some of them, such as pregnancy test kits, and blood glucose tests that patients with diabetes monitor on a regular basis (Canadian Agency for Drugs and Technologies in Health [CDA-AMC], 2024). For more information, read the section on Roche.
-
Progesterone - Progesterone is a reproductive hormone that is produced naturally in the body by both sexes. Progestin is the synthetic form of progesterone that is used in some forms of contraception methods or devices (Cleveland Clinic, 2023a). Learn more about hormones and birth control here.
-
Psychological & Psychiatric Manifestations - I detail neuropsychiatric manifestations in APS patients, which you can read more about here.
-
Pulmonary Manifestations - According to Espinosa et al. (2002):
“Patients with antiphospholipid syndrome (APS) may develop a broad spectrum of pulmonary disease. Pulmonary thromboembolism and pulmonary hypertension are the most common complications, but microvascular pulmonary thrombosis, pulmonary capillaritis, and alveolar haemorrhage have also been reported.”
Thus, APS can affect the lungs in a variety of ways that range from blood clotting to bleeding events. Always seek medical attention immediately should you suspect a blood clot in the lung, as this can be life-threatening. Learn more about APS pulmonary manifestations here.
Pin to Your Antiphospholipid Syndrome Diagnosis & Health Guide Boards:
Q is for Quinoa
I didn’t know that quinoa could be ‘dangerous’, until I ate a plateful of this healthy grain, and woke up the next day to a giant bruise that spanned my entire upper arm. I discovered that the hulls of quinoa seeds contain saponins, which is an anticoagulant (Chen et al., 2015).
Some other foods that contain saponins and thus, have a blood thinning effect (although to varying effects) are: soymilk, asparagus, strawberry, alfalfa, sea cucumber (yes, we Chinese love it), and more. For more information, read this paper in the “Food Research International” journal by Cheok et al. (2014).
In my personal experience, alfalfa sprouts are a big ‘no’ more due to Lupus and inflammatory reasons (Johns Hopkins Lupus Center, n.d.-a). Asparagus, sea cucumber, strawberries and the likes seem to be okay for me. I moderate the amount of soybean products I consume.
What your own body can and cannot tolerate is greatly dependent on your own genetics, allergies, comorbidities, diet, etc, so I cannot speak for you. It’s a shame though, because I actually like a lot of these foods, and they’re supposed to be good for you! You can learn more about warfarin interactions here.
Pin to Your Antiphospholipid Syndrome, Food & Nutrition Boards:
R is for Roche, Research & Reversal
Roche
Roche is a medical company that sells INR self-test machines called “CoaguChek®”. Many Afib (atrial fibrillation) and Antiphospholipid Syndrome patients who take warfarin use these machines to monitor their INR at home, or whilst on the go. It is important to note that Afib patients who are on warfarin differ from APS patients, as the former group may not have aPL antibodies that may further interfere with the INR reading.
There is some debate as to the accuracy of the CoaguChek (Taylor et al., 2017). This may be especially true for APS patients with elevated anti-β2GPI antibodies and are positive for lupus anticoagulant (Perry et al., 2017). It is also not recommended for patients who require an INR of 4 and above.
My Own Experiences with Roche’s CoaguChek XS & How I Use It
I personally own a CoaguChek XS (Roche Diagnostics, n.d.), and it was actually Prof. Hughes who recommended that I consider one. I can only share my personal thoughts and experiences with it, but cannot speak for all APS patients. I first discussed it with my own rheumatologist, and we then used it to test my INR right after a venous blood draw on multiple occasions.
We learned that the range difference is about +-0.3 for me, which makes it fairly stable. I also have a heart rhythm disorder, and my heart rhythm specialist has many Afib patients who take warfarin and use the machine. As she tells me, what’s important is that my INR falls within my target range, and not to hit a specific, exact number. This is because INR levels can shift throughout the day, and even with two venous blood draws or POC (point-of-care) tests done back to back.
My CoaguChek XS has been my faithful companion for many years now. Whenever I fear that my diet might have messed my INR up at home, I do a finger prick test to check. I also bring it along for all my travels, which gives me peace of mind when I don’t have regular access to my rheumatologist or blood tests.
APS Research
APS is a rare disease and more research is needed both on a global, scientific level, and also on a personal patient level (hence why I’m writing this resource page!). It is also crucial that you do your own research – from foods to medication interactions, symptom awareness and more. Every bit of knowledge can be useful in helping you manage an Antiphospholipid Syndrome diagnosis.
There is also promising research in relation to Antiphospholipid Syndrome, which I have documented and will keep updated in this post.
Reversal of Anticoagulants
Wait… but isn’t Antiphospholipid Syndrome a blood clotting disorder? Well, at present, the only management for APS is through the use of anticoagulants. These only ‘thin’ the blood, but they do not fix the root, autoimmune issue.
As a result, APS patients on blood thinners can suffer from excessive bleeding or a haemorrhage. In some instances, this can lead to a life-threatening situation, such as an ovarian cyst rupture, or after an accident. In such cases, the blood ‘thinning’ effects of the anticoagulant medication(s) need to be reversed via a reversal/hemostatic agent. Learn more about reversal agents and the reversal protocol here.
Other Terms for “R” and APS are:
-
Rare Disease - Antiphospholipid Syndrome is a rare disease, with only about 1 – 2 cases per 100,000 (Dabit et al., 2021). More diverse, population-based studies are still needed to learn more about it. Thus, raising awareness about it is extra important.
-
Rashes / Urticaria - These are some skin manifestations that can happen with an Antiphospholipid Syndrome diagnosis. Learn more about APS dermatologic manifestations here.
-
Refractory APS - Refractory Antiphospholipid Syndrome refers to cases where the patient is resistant to regular anticoagulation treatment, and can still thrombose despite being at an optimal INR range or medication dosage. Several alternative therapies such as LMWH (low molecular weight heparin), hydroxychloroquine and prednisolone have been used for various reasons, but there are currently no standardised treatment protocols for it (Scoble et al., 2011).
Here are three case studies on anticoagulant-refractory thrombotic Antiphospholipid Syndrome from Cohen and Isenberg (2021), should you be interested to learn more.
-
Rivaroxaban (Xarelto) - This is another type of DOAC under the factor Xa class. Learn more about DOACs such as rivaroxaban here.
Pin to Your Antiphospholipid Syndrome Diagnosis, Management & Treatment Boards:
S is for Strokes, Secondary APS, Surgery, Supplements & Saponins
Strokes
There are two types of strokes – ischaemic and haemorrhagic. An ischaemic stroke happens when a blood clot blocks an artery in the brain, thus restricting blood flow. A haemorrhagic stroke on the other hand, happens when a blood vessel within the brain itself bursts (CDC, 2024a). There is also something known as a ‘mini stroke’, or a transient ischaemic attack (TIA), where blood supply to the brain is temporarily disrupted. It was also my first manifestation of APS when I was 14.
If you’re more of a visual person, here’s a video on strokes by the NHLBI (2020) that explains more:
A common framework for recognising the signs and symptoms of a stroke is ‘F.A.S.T’, where the abbreviations represent (HealthHub, n.d.):
- Face drooping to one side
- Arm weakness
- Speech difficulty
- Time to call for medical help immediately
Strokes in APS Patients
Strokes are also one of the most feared consequences of Antiphospholipid Syndrome, and is particularly suspect when it happens in a young adult. According to Grimes et al. (2022):
“It has been estimated that one in five strokes and patients younger than 45 could be associated with APS and some newer studies show that APL antibodies are present in approximately 14% of stroke patients. Persistently elevated APL seems to increase the risk for CV by at least fourfold.”
And according to Novotny (n.d.):
“APS has up to five times higher prevalence among women. Symptom onset is usually between 30-40 years of age. APS-related stroke represents up to 20% of stroke events in patients under 45 years of age. In older patients, APS is less common, however, it is more prevalent in males, and stroke as a complication is more common.”
Whilst the epidemiological data varies in different papers, what one can definitely conclude is that an Antiphospholipid Syndrome diagnosis increases the chances of getting a stroke. Thus, it is important to do what you can to prevent one, such as maintaining good heart health and taking your medications as prescribed.
Learn more about strokes and transient ischaemic attacks (TIAs) in this post.
Secondary APS
Antiphospholipid Syndrome can be subdivided into three broad classifications, namely: Primary APS (PAPS), Secondary APS (SAPS) and Catastrophic APS (CAPS). PAPS is when patients only have an Antiphospholipid Syndrome diagnosis, whilst SAPS is when they have an associated autoimmune disorder such as SLE (Systemic Lupus Erythematosus). CAPS is when multiple blood clots occur simultaneously in various parts of the body in a short span of time, and has a high mortality rate (Bustamante et al., 2024).
Personally for me, it started out as PAPS, then morphed into SAPS (with Lupus, Sjögren’s disease and other chronic illnesses tailing along). Whilst APS and SLE are two different autoimmune disorders, their symptoms often overlap as well. There is also a higher risk of developing SLE within the first 5 years of an Antiphospholipid Syndrome diagnosis (Chen et al., 2021).
Having said that, these terms are merely classifications. APS patients in all categories (definitely in CAPS) can still thrombose, and should try to mitigate potential triggers. Learn more about primary and secondary manifestations in APS here.
Surgery & APS
It is vital to let your surgeon know that you are on anticoagulants before any surgery – even minor ones. This includes dental procedures, and deep tissue injections for vaccines. Healthcare professionals tend to avoid surgery with me unless it is absolutely necessary, as I am a high-risk patient for both blood clotting and bleeding incidents. The irony is that the risk for APS patients to clot during surgery can be higher than the risk from the surgical procedure itself.
According to Kim et al. (2020):
“When such patients undergo surgery, however, the underlying risk of thrombosis increases as a result of anticoagulant withdrawal, immobilization, and/or intimal injury. Conversely, there is also an increased risk of bleeding due to thrombocytopaenia, possible disseminated intravascular coagulation, or progression to catastrophic APS, as a result of excessive anticoagulation, surgery, and infection.”
Planned Surgeries
Before a planned surgery, your nurse clinician or doctor will do an anticoagulant reversal and conversion to LMWH (low molecular weight heparin) with you over the span of a few days. The LMWH is then paused about 24 hours before the surgery. This is in hope that the patient doesn’t bleed during surgery. Depending on the risk to the patient, LMWH and warfarin is then reintroduced accordingly. Learn more about LMWH and the reversal protocol in this post.
Emergency Surgeries
Emergency surgeries can be extra complicated for APS patients. I personally have had one or two emergency surgeries done before. In general, they inject you with vitamin K and/or other coagulant drugs to bring your INR back to baseline, before performing the surgery. Additional measures they may need to take are to keep the patient hydrated, use a compression machine or stockings on the patient, and to get their body moving again as soon as possible (Agaba et al., 2006).
Note that these are just a general idea on surgeries with APS; please work with your own medical team to provide the best care and surgical outcome for YOURSELF.
Supplements
Supplements are another controversial topic that gets people riled up. There are so many opinions on holistic healthcare, diet and supplements, with many people thinking that their method works best. This may be true – for them. Always remember that every person is different, including what works and doesn’t work. As human beings, we are all anomalies and enigmas, in that regard.
Anyway, in terms of research, this is an interesting paper on APS and the following supplements: vitamin D, omega-3 fatty acids, coenzyme Q10, gingerol, and isoquercetin. They display anti-inflammatory, antioxidant and/or anticoagulation properties via different pathways (Kello & Cho, 2023).
These may be beneficial if your body is working as intended. But if you’re on anticoagulants for APS or immunosuppressants for other chronic illnesses, these might actually work against you instead, as they may either dampen or amplify the effects of your medications and/or illness. I will write a separate post with more details on supplements and APS when I can! For now, you can check this post out to learn all about medication interactions with Antiphospholipid Syndrome.
Saponins & ‘Blood Thinning’ Foods
I am including saponins as a main category under “S” and Antiphospholipid Syndrome because many patients tend to focus on moderating vitamin K foods, but are less aware of blood thinning foods.
According to Olas et al. (2020):
“[Saponins] exist as secondary metabolites, occurring frequently in dicotyledonous plants and lower marine animals. Plant saponin extracts or single saponins have indicated antiplatelet and anticoagulant activity.”
Saponins also have the potential increase membrane permeabilisation and increase the bioavailability of certain drugs and vitamins (Olas et al., 2020). Another study on Panax notoginseng saponins and warfarin interaction by Qian et al. (2022) also revealed that it increases PT/INR levels, as well as the blood concentration and exposure time of warfarin, through the inhibition of enzyme CYP3A4 in the liver.
Types of Saponins
According to Oleszek and Oleszek (2021):
“Based on number of chains attached to the aglycone, they can be categorized as monodesmosides, bidesmosides, or tridesmosides.”
“Triterpenoid saponins can be found in many legumes” (such as alfafa and lentils), ginseng roots, tea leaves, quinoa seeds and much more. Steroidal saponins on the other hand can be found in oats, yucca, ginseng roots, asparagus and more.
Health-Related Properties of Saponins
Saponins can be great for general health, as they have been found to possess “immunostimulatory, hypocholesterolemic, antitumor, anti-inflammatory, antibacterial, antiviral, antifungal, and antiparasitic” properties (Oleszek & Oleszek, 2021).
However, if you’re on warfarin treatment, then you might want to moderate foods that are high in saponins due to the antithrombotic effects. If you live with other autoimmune diseases, immunostimulatory products can often trigger your disease in undesirable ways as well. After all, your immune system is already over and not underactive 🙂
Other Terms for “S” and APS are:
-
2006 Revised Sapporo Criteria - The initial Sapporo criteria was put together in 1999 and subsequently revised in 2006, based on the insights gained from research and clinical practice. Some manifestations associated with APS, such as heart valve disease, thrombocytopenia and livedo reticularis, are not included in the 2006 revised Sapporo criteria (Miyakis et al., 2006).
A review by Bobba et al. (2007) on the 2006 revised Sapporo criteria also concluded that whilst it is an improvement in terms of face and content validity as compared to its predecessor, better reliability testing is still required. For the latest APS criteria guidelines, see the section on the 2023 ACR/EULAR APS Criteria.
-
Seizures & Spasms - Refer to this section on Neuropsychiatric Manifestations in this post.
-
Seronegative - See the section on Non-Criteria APS.
-
Sexual Intercourse - You might be wondering if having an Antiphospholipid Syndrome diagnosis will impact your sex life. This is highly subjective, but you will need to be careful that it doesn’t get too rough, or risk plenty of bruises. It’s possible to get an ovarian cyst rupture if you are a female who is ovulating as well. Learn more about ovarian cyst ruptures and progestin-based contraceptives in this post.
In a very small study of 11 male APS patients, 50% of them were found to have moderate to severe erectile dysfunction as well. The causes may be multifactorial, and some speculation that thrombosis of penile vessels might contribute to it (Lopes Gallinaro et al., 2012).
-
Singaporeans with APS - There have been a few interesting studies on Singaporeans, and the differences in clinical manifestations of APS in various ethnic groups. For example, one study at Tan Tock Seng Hospital by Tan et al. (2009) found that strokes were the most common manifestation of arterial thrombosis, more so in men than women. Malays and Indians were found to have a higher rate of venous thrombosis, and Indians had the highest rate ischaemic heart disease (IHD).
-
SLE (Systemic Lupus Erythematosus) - Quite a number of patients with APS also have SLE (like me!). See the section on Lupus for more information.
-
Snake Venom - Some snake venoms work by coagulation, and others by anticoagulation. The dilute Russell viper venom time (dRVVT) is in fact, widely used in laboratories to test for lupus anticoagulant (LA). The snake venom “activates coagulation factor X, which leads to the formation of a fibrin clot”. Lupus anticoagulant prolongs dRVVT through disruption of this process (Rand & Wolgast, 2013).
And according to Pengo et al. (2017):
“dRVVT is more sensitive than other global tests employed to detect LA and is not affected by inhibitors of factor VIII or IX. The test is most successfully implemented if you observe three steps in its execution: screening, mixing, and confirmatory studies.”
RVVT is also highly sensitive to anticoagulation drugs, including VKAs (vitamin K antagonists) and DOACs (direct oral anticoagulants), which means that tests may reflect a false negative or positive for LA whilst the patient is on anticoagulant therapy (Favaloro, 2019).
Other snake venom tests used is the prothrombin-activating Taipan snake venom time (TVST), and the Ecarin clotting time (ECT) confirmatory test. These tests are insensitive to VKAs, unlike the RVVT (Hospital for Special Surgery [HSS], 2023). And just for trivia’s sake, the Ecarin test is derived from the venom of the Indian saw-scaled viper, and the Taipan snake is the most venomous snake in the world!
-
Sports - People with APS need to avoid playing certain sports, namely contact sports, due to the high risk of bruising and bleeding, which can lead to DVTs and/or excessive bleeding (Great Ormond Street Hospital, 2016).
Sports was actually the first thing that popped into my mind and overwhelmed me with grief, when I first received my Antiphospholipid Syndrome diagnosis. I loved to play basketball and football, as well as rock-climbing. I did sports not so much for health reasons, but because I enjoyed them. I struggle to this day to exercise as I dislike solo sports, and do so out of necessity, rather than pleasure.
-
‘Sticky Blood’ - Antiphospholipid Syndrome is sometimes referred to as ‘Sticky Blood Syndrome’, due to the increased tendency for the body to form blood clots (Better Health Channel, n.d.). It’s pretty much an unofficial term and not technically correct, though it can be easier to explain what APS is about to others in layman terms!
-
Stillbirth - Antiphospholipid antibodies can increase the risk of a stillbirth by threefold to fivefold (Silver et al., 2013). Learn more about stillbirth and pregnancy in this post.
-
Stop Bleed First Aid - Like any other chronically ill person, I have my own ‘mini pharmacy’ at home. As someone with an Antiphospholipid Syndrome diagnosis, my ‘pharmacy’ includes sprays and plasters that help to stop bleeding. Something like this is essential when you’re on anticoagulants, and especially when you’re travelling.
They come in various forms, such as plasters (for minor cuts), sprays, gels and powders. I personally prefer the sprays as they cover a wider surface area, and are quick and easy to use. Here are some you can get from Amazon:
-
Support Groups - Support groups can be a lifeline for chronically ill patients, regardless of what their diagnosis may be. For patients with an Antiphospholipid Syndrome diagnosis, it can feel empowering when you meet people who just ‘get’ you, and understand the struggles you face without the need to explain.
I have met a number of ‘spoonie’ friends through social media and my advocacy work, and frequently chat with them. Whilst not all of them live with Antiphospholipid Syndrome, the symptoms and struggles from our myriad chronic illnesses tend to overlap.
These are topics that the average healthy person simply won’t understand, such as chronic fatigue which can be more debilitating than chronic pain, the loss of self-identity, the sadness of being unable to work full-time, and the worries of the financial burden.
It’s important to find support groups or friends who share the same values as you however. (And IMHO, share the same type of humour!) There are also many ‘support groups’ that are more negative than positive, so you want to steer clear from those.
At the end of the day, you know what type of support works best for you, so trust your instincts. Some patients thrive from in-person support groups, whilst others might find this draining. Regardless, some form of emotional and moral support is key to thriving with any chronic illness.
If you are a chronic illness blogger, here is a support group that I’m an admin of, and which you are welcome to join: Chronic Illness Bloggers. You can also connect with me on social media here, if you like!: Facebook, Twitter/X, Instagram, Pinterest, BlueSky and SubStack.
-
Syphilis False Positive - The Wasserman test used in the past for detecting syphilis was dependent on an antibody called reagin, which reacts with cardiolipin. The biological false positive test for syphilis was actually the first recognised test for antiphospholipid antibodies, and can occur in people with autoimmune diseases such as SLE and APS (Johns Hopkins Lupus Center, n.d.).
-
Systemic - According to García-Carrasco et al. (2013):
“Antiphospholipid syndrome (APS) is a systemic autoimmune disorder defined by the persistent presence of antiphospholipid antibodies (aPL) in plasma of patients with vascular thrombosis and/or pregnancy morbidity.”
What this means is that Antiphospholipid Syndrome symptoms are not confined to one area, and can manifest anywhere within the body. APS is also often associated with autoimmune diseases such as Lupus. Learn more about the systemic implications of APS here.
Pin to Your Antiphospholipid Syndrome Signs & Symptoms Boards:
T is for Transient Ischaemic Attack (TIA) & Triple Positive
Transient Ischaemic Attack (TIA)
Strokes and Transient Ischaemic Attacks (TIAs) are the most common neuropsychiatric manifestations of Antiphospholipid Syndrome. In fact, more than 20% of strokes in patients younger than 45 years of age may be attributed to APS (Ricarte et al., 2018). A TIA was also my first manifestation and experience with APS at 14, where exactly half of my body was numb.
Symptoms of a TIA or stroke include: weakness, paralysis in the face, arm or leg, vertigo, blurry vision or blindness, slurred speech and loss of balance or coordination (Mayo Clinic, 2024). It is critical to seek help immediately, as damage can accrue over time. The bottom line being – if you feel like something, anything’s off – please just go to the dreaded A&E / ER right away. It truly is better safe than sorry in this instance, as the effects on your body and health can be for life. Learn more about TIAs in this post.
Triple Positive
To be a ‘triple positive’ APS patient means that you have all three types of antiphospholipid antibodies (aPLs) present in your body, i.e. lupus anticoagulant (LA), anticardiolipin (aCL) and anti-β2GPI. Triple positive APS patients tend to be at a higher risk for thrombosis and obstetric complications, as well as CAPS (catastrophic APS) (Laurent et al., 2023).
Of note, the lupus anticoagulant increases the tendency to clot significantly, and studies have shown a correlation for thrombosis of up to 95% confidence interval (Galli et al., 2003).
Another thing to note is that triple positivity detection can vary, depending on the methods and type of assays used for measurement. The two broad categories of assays used to diagnose APS are LA essays and ELISAs (which measure anti-β2GPI and aCL) (Krilis & Giannakopoulos, 2014). In one study of 851 patients, triple positivity detection was also found to be of statistical significance between BioPlex® 2200 and QUANTA Lite ELISA® (Chayoua et al., 2018).
Having said that, it does not mean that single or double positive patients can be less cautious. I am double positive, but my rheumatologist says that I’ve had worst APS manifestations than someone who is triple positive, even.
Other Terms for “T” and APS are:
-
Tecarfarin - Tecarfarin is a novel vitamin K antagonist (VKA) that is being developed by Cardrenal Therapeutics, and is currently in phase III clinical trials (Cardrenal Therapeutics, n.d.). Learn more about tecarfarin and VKAs here.
-
Testosterone Therapy - It is important to note that testosterone therapy (TT) can cause the blood to clot, despite sufficient anticoagulation. It is important for patients to be screened for thrombophilia (such as antiphospholipid antibodies) prior to starting TT, as the risks may outweigh the benefits. In two studies of 88 such patients, venous thromboembolism was shown to peak at 3 months after starting TT (Glueck et al., 2019).
-
Traditional Chinese Medicine - See Cupping, Traditional Chinese Medicine (TCM) & Chiropractor.
-
Thrombin - Thrombin is the “central protease in the coagulation cascade” and also “plays a role in inflammation and cellular proliferation” (Siller-Matula et al., 2017). Learn more about thrombin here.
-
Thrombocytopenia - Thrombocytopenia is a disorder where your platelet count is too low, and thus increases the risk for bleeding (NHLBI, 2022b). Learn more about thrombocytopenia here.
-
Travel - DVTs and PEs are known colloquially as “economy class syndrome”, and can happen even in healthy people who remain immobile for long periods of time whilst on a flight or in a car. Dehydration and low oxygen levels due to the high altitude are contributing factors as well. There are perhaps up to 30,000 cases of such symptomatic passengers per year in the UK (Şabanoğlu, 2021).
Other factors that increase the risk of PEs and DVTs are: advanced age, obesity, pregnancy, estrogenic drugs, extreme cold, and being in high altitude areas for prolonged periods of time (Dutta et al., 2018). Thus, it is important for people with APS to pay attention to environmental factors whilst travelling, on top of the need to keep moving and stretching whilst in transit.
Travelling is one topic you can’t read much about in research papers, as this comes from patient experience. I share my personal best travel tips in this post, and you can learn more about DVTs here.
-
Trial and Error - A lot of having an Antiphospholipid Syndrome diagnosis is figuring things out for yourself through trial and error. As a patient who has had APS for more than 20 years, I hope to reduce the amount of errors that newly diagnosed patients make, with this resource page. Many of these errors have led to detrimental lifelong consequences, some of which could have been avoided.
Having said that, there are still some things that you will need to be cautious about, and figure out on your own, such as diet and lifestyle. Remember that we are all different in terms of genetic make up, comorbidities, life duties and more. So do what’s best for yourself, and advocate for yourself as needed. Get tips on how to do personal research from credible sources here.
Pin to Your Antiphospholipid Syndrome Diagnosis & Medical Information Boards:
U is for Ultrasound
Diagnostic Ultrasound
A diagnostic ultrasound is a non-invasive imaging test that uses high-frequency sound waves instead of radiation to ‘see’ inside the body. There are a few different types of diagnostic ultrasounds, such as abdominal, kidney, thyroid and transvaginal (Cleveland Clinic, 2022b).
Patients who are on blood thinning medications can bleed internally, such as during an ovarian cyst rupture. Ultrasounds are used to detect free fluid in such instances, which can indicate an abnormal buildup of fluid in a bodily cavity. An ultrasound is what I insist on at the A&E / ER should I suspect internal bleeding. You can read more about ovarian cyst ruptures here.
Doppler & Obstetric Ultrasound
A doppler ultrasound is able to measure blood flow in addition to images, by bouncing high-frequency sound waves off red blood cells. They are used to detect blood clots, heart valve defects, aneurysms and more (Mayo Clinic, 2023d).
A history of thrombophlebitis and the second trimester doppler ultrasound is also the best predictor of late obstetric complications in APS and/or SLE patients (Le Thi Huong et al., 2006). Obstetric ultrasound evaluations are also used to detect abnormalities in foetal growth for patients with APS and/or SLE, such as in foetal growth restriction (IUGR). They are also used to evaluate amniotic fluid volume, foetal growth and morphology (Santacruz et al., 2022).
Read this post for more information on pregnancy and APS.
Pin to Your Antiphospholipid Syndrome Diagnosis:
V is for Vegetables & Vascular Manifestations
Vegetables
Certain vegetables interact with vitamin K, and can become a tricky puzzle if you’re taking warfarin. If you’re newly diagnosed with Antiphospholipid Syndrome, the first rule to remember is that green, leafy vegetables contain the highest concentration of vitamin K.
Another thing to bear in mind with an Antiphospholipid Syndrome diagnosis is that unlike heart patients who are on warfarin, your blood has an increased tendency to clot in and of itself. This does not mean that you need to avoid vitamin K entirely, as it is important for nutritional needs. You just need to take extra precautions to consume a balanced diet and to keep track of your INR levels, together with your healthcare team. (Learn more about warfarin medication interactions here.)
Vegetable oils are also an often forgotten factor when it comes to ‘vegetables’, such as soybean, canola, olive and sesame oils. These oils also contain vitamin K, and can interact with warfarin to the unwitting patient (Nutescu et al., 2006). As this topic is rather comprehensive, I will be writing a separate post all about it.
Vascular Manifestations
The vascular system is also known as the circulatory system, and comprises arteries, veins and capillaries. Together, they circulate blood and lymphatic fluid throughout the body. Vascular diseases can be caused by blood clots, genetics, inflammation and more (University of Rochester Medical Center, n.d.-b). Learn more about vascular manifestations in APS patients here.
Other Terms for “V” and APS are:
-
Vaccinations - Studies have suggested that HPV (Human Papilloma Virus) infections are more prevalent in Lupus patients, and the HPV vaccine is recommended for patients up until 25 years of age. Extra precautions must be taken by APS patients however, due to the risk of VTE (venous thromboembolism) (Ranjan et al., 2015). It is a deep intramuscular injection, which can cause bruising and bleeding.
-
Vorapaxar (Zontivity) - Vorapaxar is a novel thrombin antagonist that is approved for coronary artery disease. Specifically, it is a protease-activated receptor (PAR) antagonist, which is involved in platelet activation, and the thrombin cascade. One of the issues with Vorapaxar is its high risk of bleeding (Signorelli et al., 2018). Learn more about vorapaxar here.
-
Vitamin K Antogonists (VKAs) - These are a class of medications for the prevention and treatment of thrombosis. You might be familiar with the most well-known of the lot by now – warfarin. I write about VKAs in greater detail here.
Pin to Your Antiphospholipid Syndrome Guide Boards:
W is for Warfarin & Women
Warfarin
Warfarin is a vitamin K antagonist that inhibits multiple vitamin K dependent clotting factors, specifically factors II, VII, IX, and X, as well as the anticoagulant proteins C and S (Crader et al., 2023). In general, patients with an Antiphospholipid Syndrome diagnosis are advised to use warfarin instead of DOACs (direct oral anticoagulants) for treatment, especially if they have a history of arterial thrombosis, or are triple and even double positive (Girón-Ortega & Girón-González, 2023).
Learn all about warfarin – from how it works to interactions with other medications – in this post.
Women
Antiphospholipid Syndrome is more commonly found in women than in men, with a ratio of about 3.5:1 (Kaul et al., 2023). I have dedicated an entire post to females and Antiphospholipid Syndrome here.
Pin to Your Antiphospholipid Syndrome Diagnosis Boards:
X is for X-Rays
Whilst x-rays are not used to diagnose APS, and they cannot show a pulmonary embolism, they are still useful to rule out other possible conditions. Apart from detecting bone fractures and tumours, x-rays can also be used to detect blocked blood vessels. When used with radioactive contrast agents, x-rays can also reveal blood flow to the heart muscle, blood vessels and organs (Mayo Clinic, 2022).
Avascular necrosis (AN) can occur in patients with APS and SLE, especially those who are on steroid treatment, and/or consume alcohol excessively. Antiphospholipid antibodies and other factors may be possible contributors as well. AN patients can be asymptomatic, and x-rays don’t always show abnormalities until months after it has begun. MRIs are more useful in detecting such cases, as compared to x-rays, CT scans, and/or bone scans (Gómez-Puerta & Pons-Estel 2010).
Angiography
An angiogram is an x-ray where a contrastive agent is injected, which helps to show the shape, structure and flow of blood vessels. It can be used to check for blockages and other issues within them (Healthdirect Australia, 2023). For example, a coronary angiography may reveal blocked arteries or intracoronary organised clots. Antiphospholipid antibodies (aPLs) can cause thrombosis in normal blood vessels, due to a number of factors (Prashanth et al., 2009).
A cardiac catheterisation and angiogram is an invasive procedure, and is used to visualise the arteries in the heart. The technique is known as arteriography. It can be used to help diagnose certain conditions such as after a heart attack or angina, or to plan surgical procedures (NHS, 2022b). It has also been noted that patients with aPLs and cerebrovascular events seem to present arterial abnormalities differently as compared to the general population, when assessed via arteriography (Provenzale et al., 1998).
For more information about cerebrovascular and cardiological manifestations in APS, read this post.
Tomography / CT Scan
A CT scan is also known as a computed tomography. It uses a combination of x-rays and computer technology to generate cross-sectional images of the body. These images are more detailed than standard x-rays, and are used to diagnose tumours, blood clots, haemorrhages, and other injuries inside the body. A contrast agent may be used to help visualise soft tissues and other fine structures better (National Institute of Biomedical Imaging and Bioengineering [NIBIB], 2022).
Multislice computed tomography (MSCT) angiography is a noninvasive, and more advanced method. According to one study of 100 APS patients, it proved to be the method of choice for monitoring blood vessel changes. Their results revealed that lower extremity blood vessel lesions were more prevalent in APS patients (Saponjski et al., 2017).
Other Terms for X & APS:
-
Xarelto - This is the brand name of the DOAC, rivaroxaban. More information on DOACs, including Xarelto, can be found here.
Pin to Your Antiphospholipid Syndrome & Autoimmune Disease Boards:
Y is for Young Adults
Strokes & Transient Ischaemic Attacks (TIAs)
Strokes and heart attacks are more commonly associated with the elderly, but it is important to be aware that young adults with Antiphospholipid Syndrome can also experience them. In fact, about 10% – 15% of strokes happen to young adults (Vaccarino et al., 2019).
According to a systematic review by Sciascia et al. (2015):
“The overall aPL frequency was estimated as 17.4% (range 5%–56%) for any CVE [cerebrovascular events], 17.2% (range 2%–56%) for stroke and 11.7% (range 2%–45%) for transient ischaemic attack (TIA). The presence of aPL increased the risk for CVE by 5.48-fold (95% CI 4.42 to 6.79).”
My first manifestation of APS was a TIA at 14 years of age, and I’m lucky in a sense to get an Antiphospholipid Syndrome diagnosis shortly after. Many patients go undiagnosed or misdiagnosed for years, even decades. Meanwhile, their invisible illnesses cause pain and symptoms that are poorly managed.
Cerebral Venous Sinus Thrombosis
Cerebral Venous Sinus Thrombosis (CVST) is a rare but severe cerebrovascular disease that is often overlooked at the outset. It accounts for about 0.5% – 1% of all strokes in the adult population, but 10% – 20% of strokes in young adults (Shen et al., 2021).
APS was found to be the underlying factor for CSVT in 6% – 17% of patients. Whilst the exact reason is yet unclear, studies have suggested enhanced production of antiphospholipid antibodies (aPLs) as a possible factor. One study found that young adults were more prone to CSVT, and were mainly female (Shen et al., 2021).
In a small study of 11 primary APS patients, they concluded that CSVT may also occur in younger patients, with more extensive involvement of the venous system compared to other causes of venous thrombosis (Kim et al., 2000). Learn more about veins here.
Heart Attacks
Heart attacks are known medically as myocardial infarctions (MI), and occur when there is a decrease or complete stop of blood flow to the myocardium (the muscle layer of the heart) (Ojha & Dhamoon, 2023). An acute myocardial infarction (AMI) is when there is heart cell death during a heart attack (Sweis & Jivan, 2024).
It is important to note that young adults with APS can also suffer from AMI, due to antiphospholipid antibodies. They can also suffer from valvular abnormalities in addition to that (Osula et al., 2002).
Learn more about heart attacks and cardiovascular manifestations in APS patients here.
Pin to Your Antiphospholipid Syndrome & Chronic Illness Boards:
Z is for Zinc
To be honest, I had no idea about zinc and its interaction with phospholipids, until I had to go dig for medical terms starting with the infamous ‘Z’. Zinc is a trace mineral that can be found in food sources such as: shellfish, beef, legumes, nuts, seeds and whole grains (Harvard T.H. Chan School of Public Health, 2023).
Zinc is also available in supplement form that you can purchase over-the-counter. Only small amounts are needed by the body; consuming too much of it can be toxic. The recommended daily allowance is 8 – 11mg, and people in industrialised countries rarely have zinc deficiencies, unless they have malabsorption syndromes or are on a restricted diet (Mount Sinai, n.d.-b).
Yet, zinc occurs as constituents of more than 300 enzymes. It is involved in processes that are also altered by the action of antiphospholipid antibodies. A lack of zinc can indirectly result in inadequate blood flow, in addition to many other health issues. According to Tubek et al. (2008):
“In this regard, if antiphospholipid antibodies alter the structure and function of cell membranes of thrombocytes and endothelium then an effect on the above-mentioned phenomena could be expected. The clinical symptoms of these alterations include early atherosclerosis development, thrombosis, and pulmonary embolism.”
You can learn more about how Antiphospholipid Syndrome affects various organs and bodily systems here.
Pin to Your Antiphospholipid Syndrome & Chronic Illness Guide Boards:
Conclusion to the Antiphospholipid Syndrome Diagnosis: A – Z Guide
It is my sincere hope that this resources page has been useful to you, especially if you’ve just received an Antiphospholipid Syndrome diagnosis. As a patient, I know just how scary it can be, and the feelings of both loss and feeling lost.
I hope that this resource page can be like a small flame amidst that terrifying fog, and I have faith that you will manage it to the best of your own abilities. Sending well wishes, and feel free to leave a comment should you have more questions, a story to share, or a correction to point out. I am not a doctor, afterall 😉 Thank you so much for reading until the very end!
If you liked this resource and would like to show your token of appreciation, you can do so with the button below. Thank you for your support!
Pin to Your Antiphospholipid Syndrome Diagnosis & Chronic Illness Boards:
- Adili, R., Hawley, M., & Holinstat, M. (2018). Regulation of platelet function and thrombosis by omega-3 and omega-6 polyunsaturated fatty acids. Prostaglandins & Other Lipid Mediators, 139, 10–18. https://doi.org/10.1016/j.prostaglandins.2018.09.005
- Agaba, A., Charaklias, N., Babu-Victor, A., Agaba, P., Deepchand, V., Dabasia, H., Sharma, S., Goodrick, M., & Ramanand, B. (2006). Antiphospholipid Syndrome: A Series of Surgical Emergencies and the Current Evidence for its Management. Annals of The Royal College of Surgeons of England, 88(4), 370–374. https://doi.org/10.1308/003588406X106496
- Agrawal, A., Kerndt, C. C., & Manna, B. (2024). Apixaban. In StatPearls [Internet]. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK507910/
- Ahluwalia, J., & Sreedharanunni, S. (2017). The Laboratory Diagnosis of the Antiphospholipid Syndrome. Indian Journal of Hematology & Blood Transfusion, 33(1), 8–14. https://doi.org/10.1007/s12288-016-0739-y
- Ambati, A., Zuo, Y., & Knight, J. S. (2023). An update on inflammation in antiphospholipid syndrome (APS). Current Opinion in Rheumatology, 35(2), 89–97. https://doi.org/10.1097/BOR.0000000000000926
- American National Red Cross. (n.d.). What Are Platelets In Blood. Retrieved August 7, 2024, from https://www.redcrossblood.org/donate-blood/dlp/platelet-information.html
- APS Support UK. (n.d.). APS and women’s health. Retrieved August 1, 2024, from https://aps-support.org.uk/self-help/living-with-aps/aps-and-womens-health
- Asherson, R. A., & Cervera, R. (1994). ‘Primary’, ‘Secondary’ and Other Variants of the Antiphospholipid Syndrome. Lupus, 3(4), 293–298. https://doi.org/10.1177/096120339400300417
- Ashorobi, D., Ameer, M. A., & Fernandez, R. (2024, February 12). Thrombosis. In StatPearls [Internet]. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK538430/
- Australian Immunisation Handbook. (2023, October 23). Vaccination for people with bleeding disorders. https://immunisationhandbook.health.gov.au/contents/vaccination-for-special-risk-groups/vaccination-for-people-with-bleeding-disorders
- Barbhaiya, M., Zuily, S., Naden, R., Hendry, A., Manneville, F., Amigo, M.-C., Amoura, Z., Andrade, D., Andreoli, L., Artim-Esen, B., Atsumi, T., Avcin, T., Belmont, M. H., Bertolaccini, M. L., Branch, D. W., Carvalheiras, G., Casini, A., Cervera, R., Cohen, H., … Erkan, D. (2023). 2023 ACR/EULAR antiphospholipid syndrome classification criteria. Annals of the Rheumatic Diseases, 82(10), 1258–1270. https://doi.org/10.1136/ard-2023-224609
- Barinotti, A., Radin, M., Cecchi, I., Foddai, S. G., Rubini, E., Roccatello, D., Sciascia, S., & Menegatti, E. (2020). Genetic Factors in Antiphospholipid Syndrome: Preliminary Experience with Whole Exome Sequencing. International Journal of Molecular Sciences, 21(24), Article 24. https://doi.org/10.3390/ijms21249551
- Barnes, G. D., Ageno, W., Ansell, J., & Kaatz, S. (2015). Recommendation on the nomenclature for oral anticoagulants: Communication from the SSC of the ISTH. Journal of Thrombosis and Haemostasis, 13(6), 1154–1156. https://doi.org/10.1111/jth.12969
- Baroni, G., Banzato, A., Bison, E., Denas, G., Zoppellaro, G., & Pengo, V. (2017). The role of platelets in antiphospholipid syndrome. Platelets, 28(8), 762–766. https://doi.org/10.1080/09537104.2017.1280150
- Basaran, O., Soybilgic, A., Onel, K. B., & Erkan, D. (2020, September 2). Pediatric Antiphospholipid Syndrome | HSS Rheumatology. Hospital for Special Surgery. https://www.hss.edu/conditions_top-ten-points-pediatric-antiphospholipid-syndrome.asp
- Bertin, D., Brodovitch, A., Lopez, A., Arcani, R., Thomas, G. M., Beziane, A., Weber, S., Babacci, B., Heim, X., Rey, L., Leone, M., Mege, J. L., & Bardin, N. (2022). Anti-cardiolipin IgG autoantibodies associate with circulating extracellular DNA in severe COVID-19. Scientific Reports, 12(1), 12523. https://doi.org/10.1038/s41598-022-15969-y
- Better Health Channel. (n.d.). Hughes syndrome. Department of Health & Human Services. Retrieved August 1, 2024, from http://www.betterhealth.vic.gov.au/health/conditionsandtreatments/hughes-syndrome
- Bobba, R. S., Johnson, S. R., & Davis, A. M. (2007). A review of the sapporo and revised Sapporo criteria for the classification of antiphospholipid syndrome. Where do the revised sapporo criteria add value? The Journal of Rheumatology, 34(7), 1522–1527. https://www.jrheum.org/content/34/7/1522
- Booth, S. L., & Centurelli, M. A. (1999). Vitamin K: A Practical Guide to the Dietary Management of Patients on Warfarin. Nutrition Reviews, 57(9), 288–296. https://doi.org/10.1111/j.1753-4887.1999.tb01815.x
- Bove, R. (2013). Autoimmune diseases and reproductive aging. Clinical Immunology, 149(2), 251–264. https://doi.org/10.1016/j.clim.2013.02.010
- Bowles, L., Platton, S., Yartey, N., Dave, M., Lee, K., Hart, D. P., MacDonald, V., Green, L., Sivapalaratnam, S., Pasi, K. J., & MacCallum, P. (2020). Lupus Anticoagulant and Abnormal Coagulation Tests in Patients with Covid-19. New England Journal of Medicine, 383(3), 288–290. https://doi.org/10.1056/NEJMc2013656
- Bus, K., & Szterk, A. (2021). Relationship between Structure and Biological Activity of Various Vitamin K Forms. Foods, 10(12), Article 12. https://doi.org/10.3390/foods10123136
- Bustamante, J. G., Goyal, A., Rout, P., & Singhal, M. (2024, May 6). Antiphospholipid Syndrome. In StatPearls [Internet]. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK430980/
- Cadrenal Therapeutics, Inc. (n.d.). Tecarfarin—A late-stage novel therapy with orphan drug and Fast Track designations. Retrieved August 1, 2024, from https://www.cadrenal.com/tecarfarin/
- Canadian Agency for Drugs and Technologies in Health. (2024, July 31). 2. Point-of-Care Testing. https://www.cadth.ca/2-point-care-testing
- Caporuscio, J. (2021, February 25). What to know about blood thinners and alcohol. Medical News Today. https://www.medicalnewstoday.com/articles/blood-thinners-and-alcohol
- Capozzi, A., Riitano, G., Mancuso, S., Recalchi, S., Manganelli, V., Garofalo, T., Alessandri, C., Longo, A., Misasi, R., Conti, F., Truglia, S., & Sorice, M. (2021). Anti‐vimentin/cardiolipin IgA in the anti‐phospholipid syndrome: A new tool for ‘seronegative’ diagnosis. Clinical and Experimental Immunology, 205(3), 326–332. https://doi.org/10.1111/cei.13633
- Castro-Marrero, J., Balada, E., Vilardell-Tarrés, M., & Ordi-Ros, J. (2009). Genetic risk factors of thrombosis in the antiphospholipid syndrome. British Journal of Haematology, 147(3), 289–296. https://doi.org/10.1111/j.1365-2141.2009.07831.x
- Centers for Disease Control and Prevention [CDC]. (n.d.). Lupus Basics. Retrieved August 1, 2024, from https://www.cdc.gov/lupus/about/index.html
- Centers for Disease Control and Prevention [CDC]. (2021, November 16). Administering HPV Vaccine. https://www.cdc.gov/vaccines/vpd/hpv/hcp/administration.html
- Centers for Disease Control and Prevention [CDC]. (2024a, May 15). About Stroke. https://www.cdc.gov/stroke/about/index.html
- Centers for Disease Control and Prevention [CDC]. (2024b, May 16). About Hemophilia. https://www.cdc.gov/hemophilia/about/index.html
- Cervera, R. (2008). Lessons from the “Euro-Phospholipid” project. Autoimmunity Reviews, 7(3), 174–178. https://doi.org/10.1016/j.autrev.2007.11.011
- Cervera, R., Asherson, R., Acevedo, M., Gomez-Puerta, J., Espinosa, G., de la Red, G., Gil, V., Ramos-Casals, M., Garcia-Carrasco, M., Ingelmo, M., & Font, J. (2004). Antiphospholipid syndrome associated with infections: Clinical and microbiological characteristics of 100 patients. Annals of the Rheumatic Diseases, 63(10), 1312–1317. https://doi.org/10.1136/ard.2003.014175
- Cervera, R., Conti, F., Doria, A., Iaccarino, L., & Valesini, G. (2012). Does seronegative antiphospholipid syndrome really exist? Autoimmunity Reviews, 11(8), 581–584. https://doi.org/10.1016/j.autrev.2011.10.017
- Cervera, R., Piette, J.-C., Font, J., Khamashta, M. A., Shoenfeld, Y., Camps, M. T., Jacobsen, S., Lakos, G., Tincani, A., Kontopoulou-Griva, I., Galeazzi, M., Meroni, P. L., Derksen, R. H. W. M., de Groot, P. G., Gromnica-Ihle, E., Baleva, M., Mosca, M., Bombardieri, S., Houssiau, F., … Ingelmo, M. (2002). Antiphospholipid syndrome: Clinical and immunologic manifestations and patterns of disease expression in a cohort of 1,000 patients. Arthritis & Rheumatism, 46(4), 1019–1027. https://doi.org/10.1002/art.10187
- Cervera, R., Rodríguez-Pintó, I., & Espinosa, G. (2018). The diagnosis and clinical management of the catastrophic antiphospholipid syndrome: A comprehensive review. Journal of Autoimmunity, 92, 1–11. https://doi.org/10.1016/j.jaut.2018.05.007
- Chayoua, W., Kelchtermans, H., Moore, G. W., Musiał, J., Wahl, D., de Laat, B., & Devreese, K. M. J. (2018). Identification of high thrombotic risk triple‐positive antiphospholipid syndrome patients is dependent on anti‐cardiolipin and anti‐β2glycoprotein I antibody detection assays. Journal of Thrombosis and Haemostasis, 16(10), 2016–2023. https://doi.org/10.1111/jth.14261
- Chen, C., Yang, F.-Q., Zhang, Q., Wang, F.-Q., Hu, Y.-J., & Xia, Z.-N. (2015). Natural Products for Antithrombosis. Evidence-Based Complementary and Alternative Medicine : eCAM, 2015, 876426. https://doi.org/10.1155/2015/876426
- Chen, H.-H., Lin, C.-H., & Chao, W.-C. (2021). Risk of Systemic Lupus Erythematosus in Patients With Anti-phospholipid Syndrome: A Population-Based Study. Frontiers in Medicine, 8, 654791. https://doi.org/10.3389/fmed.2021.654791
- Cheok, C. Y., Salman, H. A. K., & Sulaiman, R. (2014). Extraction and quantification of saponins: A review. Food Research International, 59, 16–40. https://doi.org/10.1016/j.foodres.2014.01.057
- Chua, Y. T., Ang, X. L., Zhong, X. M., & Khoo, K. S. (2015). Interaction between warfarin and Chinese herbal medicines. Singapore Medical Journal, 56(1), 11–18. https://doi.org/10.11622/smedj.2015004
- Churchill, J., & Gudgel, D. T. (2024, February 24). What Is an Ophthalmologist vs Optometrist? American Academy of Ophthalmology. https://www.aao.org/eye-health/tips-prevention/what-is-ophthalmologist
- Cleveland Clinic. (n.d.). Etonogestrel Implant. Retrieved August 1, 2024, from https://my.clevelandclinic.org/health/drugs/18407-etonogestrel-implant
- Cleveland Clinic. (2022a, January 10). Anticoagulants. https://my.clevelandclinic.org/health/treatments/22288-anticoagulants
- Cleveland Clinic. (2022b, April 12). Ultrasound. https://my.clevelandclinic.org/health/diagnostics/4995-ultrasound
- Cleveland Clinic. (2022c, May 5). Antiplatelet Drugs. https://my.clevelandclinic.org/health/drugs/22955-antiplatelet-drugs
- Cleveland Clinic. (2022d, July 12). Blood Disorders. https://my.clevelandclinic.org/health/diseases/21545-blood-disorders
- Cleveland Clinic. (2023a, March 21). Progestin. https://my.clevelandclinic.org/health/treatments/24838-progestin
- Cleveland Clinic. (2023b, April 18). Intermittent Pneumatic Compression. https://my.clevelandclinic.org/health/treatments/14791-intermittent-pneumatic-compression-ipc-device
- Cleveland Clinic. (2024a, February 20). What Is a Pulmonary Embolism? https://my.clevelandclinic.org/health/diseases/17400-pulmonary-embolism
- Cleveland Clinic. (2024b, April 19). Embolism. https://my.clevelandclinic.org/health/diseases/embolism
- Cohen, H., & Isenberg, D. A. (2021). How I treat anticoagulant-refractory thrombotic antiphospholipid syndrome. Blood, 137(3), 299–309. https://doi.org/10.1182/blood.2020004942
- Cojocaru, M., Cojocaru, I. M., & Silosi, I. (2010). Multiple autoimmune syndrome. Mædica, 5(2), 132–134. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3150011/
- Cook, B. W. (2010). Anticoagulation Management. Seminars in Interventional Radiology, 27(4), 360–367. https://doi.org/10.1055/s-0030-1267849
- Crader, M. F., Johns, T., & Arnold, J. K. (2023, May 1). Warfarin Drug Interactions. In StatPearls [Internet]. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK441964/
- Dabit, J. Y., Valenzuela-Almada, M. O., Vallejo-Ramos, S., & Duarte-García, A. (2021). Epidemiology of Antiphospholipid Syndrome in the General Population. Current Rheumatology Reports, 23(12), 85. https://doi.org/10.1007/s11926-021-01038-2
- de Carvalho, J. F. (2011). Influence of gender on the clinical and laboratory spectra of patients with primary antiphospholipid syndrome. Rheumatology International, 31(5), 647–650. https://doi.org/10.1007/s00296-009-1346-0
- Delgado, B. J., & Lopez-Ojeda, W. (2023, June 26). Estrogen. In StatPearls [Internet]. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK538260/
- Devreese, K. M. J., Groot, P. G. de, Laat, B. de, Erkan, D., Favaloro, E. J., Mackie, I., Martinuzzo, M., Ortel, T. L., Pengo, V., Rand, J. H., Tripodi, A., Wahl, D., & Cohen, H. (2020). Guidance from the Scientific and Standardization Committee for lupus anticoagulant/antiphospholipid antibodies of the International Society on Thrombosis and Haemostasis. Journal of Thrombosis and Haemostasis, 18(11), 2828–2839. https://doi.org/10.1111/jth.15047
- Di Prima, F. A. F., Valenti, O., Hyseni, E., Giorgio, E., Faraci, M., Renda, E., De Domenico, R., & Monte, S. (2011). Antiphospholipid Syndrome during pregnancy: The state of the art. Journal of Prenatal Medicine, 5(2), 41–53. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3279165/
- DiNicolantonio, J. J., & OKeefe, J. (2019). Importance of maintaining a low omega-6/omega-3 ratio for reducing platelet aggregation, coagulation and thrombosis. Open Heart, 6(1), e001011. https://doi.org/10.1136/openhrt-2019-001011
- Drini, M. (2017). Peptic ulcer disease and non-steroidal anti-inflammatory drugs. Australian Prescriber, 40(3), 91–93. https://doi.org/10.18773/austprescr.2017.037
- DrugBank Online. (n.d.). Drug Interaction Checker. Retrieved August 1, 2024, from https://go.drugbank.com/drug-interaction-checker
- Drugs .com. (n.d.). Enoxaparin (Ingredient). Retrieved August 1, 2024, from https://www.drugs.com/ingredient/enoxaparin.html
- Dutta, V., Singh, R., Kumar, S., Aggarwal, N., & Hari Kumar, K. V. S. (2018). Profile of pulmonary embolism in service personnel posted at high altitude area. Indian Heart Journal, 70(3), 427–429. https://doi.org/10.1016/j.ihj.2017.08.002
- Erkan, D., Erel, H., Yazici, Y., & Prince, M. R. (2002). The role of cardiac magnetic resonance imaging in antiphospholipid syndrome. The Journal of Rheumatology, 29(12), 2658–2659. https://www.jrheum.org/content/29/12/2658
- Espinosa, G., Cervera, R., Font, J., & Asherson, R. A. (2002). The lung in the antiphospholipid syndrome. Annals of the Rheumatic Diseases, 61(3), 195–198. https://doi.org/10.1136/ard.61.3.195
- Exploring Our Fluid Earth. (n.d.). Practices of Science: False Positives and False Negatives. University of Hawai‘i. Retrieved August 1, 2024, from https://manoa.hawaii.edu/exploringourfluidearth/chemical/matter/properties-matter/practices-science-false-positives-and-false-negatives
- Farag, M. A., & Gad, M. Z. (2022). Omega-9 fatty acids: Potential roles in inflammation and cancer management. Journal of Genetic Engineering & Biotechnology, 20, 48. https://doi.org/10.1186/s43141-022-00329-0
- Favaloro, E. J. (2019). The Russell viper venom time (RVVT) test for investigation of lupus anticoagulant (LA). American Journal of Hematology, 94(11), 1290–1296. https://doi.org/10.1002/ajh.25606
- Favaloro, E. J., Pasalic, L., & Lippi, G. (2023). Classification Criteria for the Antiphospholipid Syndrome: Not the Same as Diagnostic Criteria for Antiphospholipid Syndrome. Seminars in Thrombosis and Hemostasis, 50, 605–608. https://doi.org/10.1055/s-0043-1776318
- Furhad, S., Sina, R. E., & Bokhari, A. A. (2023). Cupping Therapy. In StatPearls [Internet]. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK538253/
- Fusaro, M., Mereu, M. C., Aghi, A., Iervasi, G., & Gallieni, M. (2017). Vitamin K and bone. Clinical Cases in Mineral and Bone Metabolism, 14(2), 200–206. https://doi.org/10.11138/ccmbm/2017.14.1.200
- Galli, M., Luciani, D., Bertolini, G., & Barbui, T. (2003a). Lupus anticoagulants are stronger risk factors for thrombosis than anticardiolipin antibodies in the antiphospholipid syndrome: A systematic review of the literature. Blood, 101(5), 1827–1832. https://doi.org/10.1182/blood-2002-02-0441
- García-Carrasco, M., Pinto, C. M., Hernández, C. J., Poblano, J. C. S., Morales, I. E., & Martínez, S. M. (2013). Antiphospholipid syndrome. In Autoimmunity: From Bench to Bedside [Internet]. El Rosario University Press. https://www.ncbi.nlm.nih.gov/books/NBK459442/
- Garrard, A. (2014). Coumarins. In P. Wexler (Ed.), Encyclopedia of Toxicology (Third Edition) (pp. 1052–1054). Academic Press. https://doi.org/10.1016/B978-0-12-386454-3.00798-3
- Gezer, S. (2003). Antiphospholipid syndrome. Disease-a-Month, 49(12), 696–741. https://doi.org/10.1016/j.disamonth.2003.10.001
- Gibson, G. E., Daniel Su, W. P., & Pittelkow, M. R. (1997). Antiphospholipid syndrome and the skin. Journal of the American Academy of Dermatology, 36(6), 970–982. https://doi.org/10.1016/S0190-9622(97)80283-6
- Girón-Ortega, J. A., & Girón-González, J. A. (2023). Direct-acting oral anticoagulants in antiphospholipid syndrome: A systematic review. Medicina Clínica (English Edition), 161(2), 65–77. https://doi.org/10.1016/j.medcle.2023.03.017
- Glueck, C. J., Goldenberg, N., & Wang, P. (2019). Testosterone Therapy, Thrombophilia, Venous Thromboembolism, and Thrombotic Events. Journal of Clinical Medicine, 8(1), Article 1. https://doi.org/10.3390/jcm8010011
- Gómez-Puerta, J. A., & Cervera, R. (2014). Diagnosis and classification of the antiphospholipid syndrome. Journal of Autoimmunity, 48–49, 20–25. https://doi.org/10.1016/j.jaut.2014.01.006
- Gomez-Puerta, J. A., & Pons-Estel, G. (2010). Skeletal Involvement in Antiphospholipid Syndrome. Current Rheumatology Reviews, 6(1), 25–31. https://doi.org/10.2174/157339710790827722
- Grayson, L., Vines, B., Nichol, K., & Szaflarski, J. P. (2017). An interaction between warfarin and cannabidiol, a case report. Epilepsy & Behavior Case Reports, 9, 10–11. https://doi.org/10.1016/j.ebcr.2017.10.001
- Great Ormond Street Hospital for Children. (2016, December). Warfarin. NHS Foundation Trust. https://www.gosh.nhs.uk/conditions-and-treatments/medicines-information/warfarin/
- Green, D. (2022). Pathophysiology of Antiphospholipid Syndrome. Thrombosis and Haemostasis, 122(7), 1085–1095. https://doi.org/10.1055/a-1701-2809
- Grimes, K., Klein, A. P., Lalla, R., Morawo, A., Somani, S., Woodward, M. J., Cole, J. W., Grimes, K., Klein, A. P., Lalla, R., Morawo, A., Somani, S., Woodward, M. J., & Cole, J. W. (2022). Antiphospholipid Syndrome and Stroke. IntechOpen. https://doi.org/10.5772/intechopen.101777
- Gruel, Y., De Maistre, E., Pouplard, C., Mullier, F., Susen, S., Roullet, S., Blais, N., Le Gal, G., Vincentelli, A., Lasne, D., Lecompte, T., Albaladejo, P., Godier, A., Albaladejo, P., Belisle, S., Blais, N., Bonhomme, F., Borel-Derlon, A., Borg, J. Y., … Zufferey, P. (2020). Diagnosis and management of heparin-induced thrombocytopenia. Anaesthesia Critical Care & Pain Medicine, 39(2), 291–310. https://doi.org/10.1016/j.accpm.2020.03.012
- Hanley, J. P. (2004). Warfarin reversal. Journal of Clinical Pathology, 57(11), 1132–1139. https://doi.org/10.1136/jcp.2003.008904
- Harvard Medical School. (2019a, August 20). No need to avoid healthy omega-6 fats. Harvard Health Publishing. https://www.health.harvard.edu/newsletter_article/no-need-to-avoid-healthy-omega-6-fats
- Harvard Medical School. (2019b, December 16). Bad mix: Blood thinners and NSAIDs. Harvard Health Publishing. https://www.health.harvard.edu/diseases-and-conditions/bad-mix-blood-thinners-and-nsaids
- Harvard Medical School. (2021a, September 13). Vitamin D and your health: Breaking old rules, raising new hopes. Harvard Health Publishing. https://www.health.harvard.edu/staying-healthy/vitamin-d-and-your-health-breaking-old-rules-raising-new-hopes
- Harvard Medical School. (2021b, September 16). Osteopenia: When you have weak bones, but not osteoporosis. Harvard Health Publishing. https://www.health.harvard.edu/womens-health/osteopenia-when-you-have-weak-bones-but-not-osteoporosis
- Harzallah, I., Debliquis, A., & Drénou, B. (2020). Lupus anticoagulant is frequent in patients with Covid‐19. Journal of Thrombosis and Haemostasis, 18(8), 2064–2065. https://doi.org/10.1111/jth.14867
- Healthdirect Australia Limited. (2022, December). International normalised ratio (INR) test. Healthdirect Australia Limited. https://www.healthdirect.gov.au/international-normalised-ratio-INR-test
- HealthHub. (n.d.). You can spot a stroke. Retrieved August 1, 2024, from https://www.healthhub.sg/programmes/aap/stroke
- Hickey, M. (2023, April 28). Why Is Hemophilia Called the Royal Disease? National Bleeding Disorders Foundation. https://hemaware.org/bleeding-disorders-z/royal-disease
- Hospital for Special Surgery [HSS]. (2023, November 13). New Antiphospholipid Syndrome Research Findings Presented at ACR Convergence 2023. https://news.hss.edu/new-antiphospholipid-syndrome-research-findings-presented-at-acr-convergence-2023/
- Hoxha, A., Banzato, A., Ruffatti, A., & Pengo, V. (2017). Detection of lupus anticoagulant in the era of direct oral anticoagulants. Autoimmunity Reviews, 16(2), 173–178. https://doi.org/10.1016/j.autrev.2016.12.010
- Huang, S., Ninivaggi, M., Chayoua, W., & de Laat, B. (2021). VWF, Platelets and the Antiphospholipid Syndrome. International Journal of Molecular Sciences, 22(8), Article 8. https://doi.org/10.3390/ijms22084200
- Hughes, G. (2007). Hughes syndrome. Clinical Reviews in Allergy & Immunology, 32(1), 3–11. https://doi.org/10.1007/BF02686077
- Hughes, G. R. V. (2003). Migraine, memory loss, and “multiple sclerosis ”. Neurological features of the antiphospholipid (Hughes’) syndrome. Postgraduate Medical Journal, 79(928), 81–83. https://doi.org/10.1136/pmj.79.928.81
- Hull, R. D., Garcia, D. A., & Vazquez, S. R. (2024, June). Patient education: Warfarin (Beyond the Basics). UpToDate. https://www.uptodate.com/contents/warfarin-beyond-the-basics
- Jaffer, A., & Bragg, L. (2003). Practical tips for warfarin dosing and monitoring. Cleveland Clinic Journal of Medicine, 70(4), 361–371. https://www.ccjm.org/content/70/4/361
- Jara, L. J., Medina, G., Vera-Lastra, O., & Barile, L. (2005). The impact of gender on clinical manifestations of primary antiphospholipid syndrome. Lupus, 14(8), 607–612. https://doi.org/10.1191/0961203305lu2176oa
- Johns Hopkins Lupus Center. (n.d.-a). 5 Things to Avoid if You Have Lupus. Retrieved August 1, 2024, from https://www.hopkinslupus.org/lupus-info/lifestyle-additional-information/avoid/
- Johns Hopkins Lupus Center. (n.d.-b). Antiphospholipid Antibodies. Retrieved August 1, 2024, from https://www.hopkinslupus.org/lupus-info/lupus-affects-body/antiphospholipid-antibodies/
- Kaul, A., Jawad, A., & Hughes, G. (2023). Antiphospholipid syndrome, thrombosis and multidisciplinary management. Trends in Urology & Men’s Health, 14(3), 31–35. https://doi.org/10.1002/tre.911
- Kello, N., & Cho, Y. M. (2024). Natural supplements in antiphospholipid syndrome: A case for further study. Clinical Immunology, 258, 109848. https://doi.org/10.1016/j.clim.2023.109848
- Kim, J. H., Choi, C.-G., Choi, S.-J., Lee, H. K., & Suh, D. C. (2000). Primary Antiphospholipid Antibody Syndrome: Neuroradiologic Findings in 11 Patients. Korean Journal of Radiology, 1(1), 5–10. https://doi.org/10.3348/kjr.2000.1.1.5
- Kim, J. W., Kim, T. W., Ryu, K. H., Park, S. G., Jeong, C. Y., & Park, D. H. (2020). Anaesthetic considerations for patients with antiphospholipid syndrome undergoing non-cardiac surgery. Journal of International Medical Research, 48(1), 0300060519896889. https://doi.org/10.1177/0300060519896889
- Koliadenko, D., & Iaremenko, O. (2024). Pos0727 Validation of 2023 Acr/Eular Antiphospholipid Syndrome Classification Criteria in Patients with Systemic Lupus Erythematosus and Positive Antiphospholipid Antibodies. Annals of the Rheumatic Diseases, 83(Suppl 1), 542–543. https://doi.org/10.1136/annrheumdis-2024-eular.4562
- Krilis, S. A., & Giannakopoulos, B. (2014). Laboratory methods to detect antiphospholipid antibodies. Hematology, 2014(1), 321–328. https://doi.org/10.1182/asheducation-2014.1.321
- Kubisz, P., Holly, P., Stasko, J., Kubisz, P., Holly, P., & Stasko, J. (2021). Bleeding in Patients with Antiphospholipid Antibodies. In P. Žigon (Ed.), Antiphospholipid Syndrome—Recent Advances in Clinical and Basic Aspects. IntechOpen. https://doi.org/10.5772/intechopen.97856
- L. Booth, S. (2012). Vitamin K: Food composition and dietary intakes. Food & Nutrition Research, 56(1), 5505. https://doi.org/10.3402/fnr.v56i0.5505
- Lai, Y., Masatoshi, H., Ma, Y., Guo, Y., & Zhang, B. (2022). Role of Vitamin K in Intestinal Health. Frontiers in Immunology, 12. https://doi.org/10.3389/fimmu.2021.791565
- Laurent, C., Ricard, L., Nguyen, Y., Boffa, J. J., Rondeau, E., Gerotziafas, G., Elalamy, I., Deriaz, S., Moreuil, C. D., Planche, V., Johanet, C., Millot, F., Fain, O., & Mekinian, A. (2023). Triple positive profile in antiphospholipid syndrome: Prognosis, relapse and management from a retrospective multicentre study. RMD Open, 9(1), e002534. https://doi.org/10.1136/rmdopen-2022-002534
- Le Thi Huong, D., Wechsler, B., Vauthier-Brouzes, D., Duhaut, P., Costedoat, N., Andreu, M. R., Lefebvre, G., & Piette, J.-C. (2006). The second trimester Doppler ultrasound examination is the best predictor of late pregnancy outcome in systemic lupus erythematosus and/or the antiphospholipid syndrome. Rheumatology, 45(3), 332–338. https://doi.org/10.1093/rheumatology/kei159
- Lindley, K. J., Limdi, N. A., Cavallari, L. H., Perera, M. A., Lenzini, P., Johnson, J. A., Wu, A. H. B., Ridker, P. M., King, C. R., Eby, C. S., Patel, S., Shah, S. V., Beasley, T. M., Li, J., & Gage, B. F. (2022). Warfarin Dosing in Patients With CYP2C9*5 Variant Alleles. Clinical Pharmacology & Therapeutics, 111(4), 950–955. https://doi.org/10.1002/cpt.2549
- Liu, X., Zhu, L., Liu, H., Cai, Q., Yun, Z., Sun, F., Jia, Y., Guo, J., & Li, C. (2022). Non-criteria antiphospholipid antibodies in antiphospholipid syndrome: Diagnostic value added. Frontiers in Immunology, 13. https://doi.org/10.3389/fimmu.2022.972012
- Lockshin, M. D., Sammaritano, L. R., & Schwartzman, S. (2000). Validation of the Sapporo criteria for antiphospholipid syndrome. Arthritis & Rheumatism, 43(2), 440–443. https://doi.org/10.1002/1529-0131(200002)43:2<440::AID-ANR26>3.0.CO;2-N
- Lopes Gallinaro, A., Silva, C., Rabelo Junior, C., Correia Caleiro, M., & de Carvalho, J. (2012). Moderate/severe erectile dysfunction in patients with antiphospholipid syndrome. Lupus, 21(3), 319–323. https://doi.org/10.1177/0961203311427552
- Lu, P.-H., Liao, T.-H., Chen, Y.-H., Hsu, Y.-L., Kuo, C.-Y., Chan, C.-C., Wang, L.-K., Chern, C.-Y., & Tsai, F.-M. (2022). Coumarin Derivatives Inhibit ADP-Induced Platelet Activation and Aggregation. Molecules, 27(13), Article 13. https://doi.org/10.3390/molecules27134054
- Mansoori, B., & Herrmann, K. A. (2013). Mesentery, Omentum, Peritoneum: Fluid Collections (Ascites, Abscess, Hemorrhage). In B. Hamm & P. R. Ros (Eds.), Abdominal Imaging (pp. 1601–1622). Springer. https://doi.org/10.1007/978-3-642-13327-5_175
- Martirosyan, A., Aminov, R., & Manukyan, G. (2019). Environmental Triggers of Autoreactive Responses: Induction of Antiphospholipid Antibody Formation. Frontiers in Immunology, 10. https://doi.org/10.3389/fimmu.2019.01609
- Marzooq, F. A. (2023). Pediatric Antiphospholipid Syndrome Presenting as a Massive Stroke: A Case Report. Cureus, 15. https://doi.org/10.7759/cureus.43834
- Mayo Clinic. (2022, December 1). Pulmonary embolism. https://www.mayoclinic.org/diseases-conditions/pulmonary-embolism/diagnosis-treatment/drc-20354653
- Mayo Clinic. (2023a, July 19). Symptoms—Blood clots. https://www.mayoclinic.org/symptoms/blood-clots/basics/causes/sym-20050850
- Mayo Clinic. (2023b, July 28). Ovarian cysts. https://www.mayoclinic.org/diseases-conditions/ovarian-cysts/symptoms-causes/syc-20353405
- Mayo Clinic. (2023c, September 9). MRI. https://www.mayoclinic.org/tests-procedures/mri/about/pac-20384768
- Mayo Clinic. (2023d, December 5). Doppler ultrasound: What is it used for? https://www.mayoclinic.org/doppler-ultrasound/expert-answers/faq-20058452
- Mayo Clinic. (2024, February 9). Transient ischemic attack (TIA). https://www.mayoclinic.org/diseases-conditions/transient-ischemic-attack/symptoms-causes/syc-20355679
- McDonnell, T., Wincup, C., Buchholz, I., Pericleous, C., Giles, I., Ripoll, V., Cohen, H., Delcea, M., & Rahman, A. (2020). The role of beta-2-glycoprotein I in health and disease associating structure with function: More than just APS. Blood Reviews, 39, 100610. https://doi.org/10.1016/j.blre.2019.100610
- MedlinePlus. (2018, September 1). CYP2C9 gene. National Library of Medicine. https://medlineplus.gov/genetics/gene/cyp2c9/
- MedlinePlus. (2022a, May 8). Arterial embolism. A.D.A.M., Inc. https://medlineplus.gov/ency/article/001102.htm
- MedlinePlus. (2022b, July 11). Antiphospholipid syndrome. National Library of Medicine. https://medlineplus.gov/genetics/condition/antiphospholipid-syndrome/
- MedlinePlus. (2023, October 28). Subcutaneous (SQ) injections. A.D.A.M. Inc. https://medlineplus.gov/ency/patientinstructions/000430.htm
- MedlinePlus. (2024, May 15). Prothrombin Time Test and INR (PT/INR). National Library of Medicine. https://medlineplus.gov/lab-tests/prothrombin-time-test-and-inr-ptinr/
- Medscape. (n.d.). Drug Interactions Checker. Retrieved August 1, 2024, from https://reference.medscape.com/drug-interactionchecker
- Mendoza-Pinto, C., García-Carrasco, M., & Cervera, R. (2018). Role of Infectious Diseases in the Antiphospholipid Syndrome (Including Its Catastrophic Variant). Current Rheumatology Reports, 20(10), 62. https://doi.org/10.1007/s11926-018-0773-x
- Miyakis, S., Lockshin, M. D., Atsumi, T., Branch, D. W., Brey, R. L., Cervera, R., Derksen, R. H. W. M., De groot, P. G., Koike, T., Meroni, P. L., Reber, G., Shoenfeld, Y., Tincani, A., Vlachoyiannopoulos, P. G., & Krilis, S. A. (2006). International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). Journal of Thrombosis and Haemostasis, 4(2), 295–306. https://doi.org/10.1111/j.1538-7836.2006.01753.x
- Morad, C. S., Fayez, D., Mahmoud, M., & Aboud, F. M. (2022). Primary and secondary antiphospholipid syndrome characteristics in an Egyptian cohort. The Egyptian Rheumatologist, 44(4), 373–376. https://doi.org/10.1016/j.ejr.2022.07.006
- Mount Sinai. (n.d.-a). Green tea—Camellia sinensis. Retrieved August 1, 2024, from https://www.mountsinai.org/health-library/herb/green-tea
- Mount Sinai. (n.d.-b). Zinc. Retrieved August 1, 2024, from https://www.mountsinai.org/health-library/supplement/zinc
- Murthy, V., Willis, R., Romay-Penabad, Z., Ruiz-Limón, P., Martínez-Martínez, L. A., Jatwani, S., Jajoria, P., Seif, A., Alarcón, G. S., Papalardo, E., Liu, J., Vilá, L. M., McGwin Jr., G., McNearney, T. A., Maganti, R., Sunkureddi, P., Parekh, T., Tarantino, M., Akhter, E., … Pierangeli, S. S. (2013). Value of Isolated IgA Anti–β2-Glycoprotein I Positivity in the Diagnosis of the Antiphospholipid Syndrome. Arthritis & Rheumatism, 65(12), 3186–3193. https://doi.org/10.1002/art.38131
- Nagano, M., Kubota, K., Sakata, A., Nakamura, R., Yoshitomi, T., Wakui, K., & Yoshimoto, K. (2023). A neutralizable dimeric anti-thrombin aptamer with potent anticoagulant activity in mice. Molecular Therapy - Nucleic Acids, 33, 762–772. https://doi.org/10.1016/j.omtn.2023.07.038
- National Bleeding Disorders Foundation. (n.d.-a). Hemophilia A. Retrieved August 1, 2024, from https://www.bleeding.org/bleeding-disorders-a-z/types/hemophilia-a
- National Bleeding Disorders Foundation. (n.d.-b). Hemophilia B. Retrieved August 1, 2024, from https://www.bleeding.org/bleeding-disorders-a-z/types/hemophilia-b
- National Heart, Lung, and Blood Institute [NHLBI]. (2020, April 22). Learn About the Types of Strokes [Video]. https://www.youtube.com/watch?v=UJ5aO4KmQ8M
- National Heart, Lung, and Blood Institute [NHLBI]. (2022a, March 24). Blood Clotting Disorders—Antiphospholipid Syndrome (APS). https://www.nhlbi.nih.gov/health/antiphospholipid-syndrome
- National Heart, Lung, and Blood Institute [NHLBI]. (2022b, March 24). Platelet Disorders—Thrombocytopenia. National Institutes of Health. https://www.nhlbi.nih.gov/health/thrombocytopenia
- National Institute of Biomedical Imaging and Bioengineering [NIBIB]. (2022, June). Computed Tomography (CT). National Institutes of Health. https://www.nibib.nih.gov/science-education/science-topics/computed-tomography-ct
- National Institute of Arthritis and Musculoskeletal and Skin Diseases [NIAMS]. (2023, May). Calcium and Vitamin D: Important for Bone Health. https://www.niams.nih.gov/health-topics/calcium-and-vitamin-d-important-bone-health
- Nexplanon. (n.d.). NEXPLANON® (etonogestrel implant) 68 mg Radiopaque ǀ Official Site. Retrieved August 1, 2024, from https://www.nexplanon.com/
- Ng, H. J., & Crowther, M. A. (2006). Azathioprine and inhibition of the anticoagulant effect of warfarin: Evidence from a case report and a literature review. The American Journal of Geriatric Pharmacotherapy, 4(1), 75–77. https://doi.org/10.1016/j.amjopharm.2006.03.001
- NHS. (2022a, June 20). Causes—Antiphospholipid syndrome (APS). https://www.nhs.uk/conditions/antiphospholipid-syndrome/causes/
- NHS. (2022b, October 4). Cardiac catheterisation and coronary angiography. https://www.nhs.uk/conditions/coronary-angiography/
- Nicolas, D., Nicolas, S., Hodgens, A., & Reed, M. (2023, May 16). Heparin-Induced Thrombocytopenia. In StatPearls [Internet]. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK482330/
- Norwood, D. A., Parke, C. K., & Rappa, L. R. (2015). A Comprehensive Review of Potential Warfarin-Fruit Interactions. Journal of Pharmacy Practice, 28(6), 561–571. https://doi.org/10.1177/0897190014544823
- Noureldine, M. H. A., Khamashta, M. A., Merashli, M., Sabbouh, T., Hughes, G. R. V., & Uthman, I. (2016). Musculoskeletal manifestations of the antiphospholipid syndrome. Lupus, 25(5), 451–462. https://doi.org/10.1177/0961203316636467
- Novotny, V. (n.d.). Antiphospholipid Syndrome and Stroke. European Stroke Organisation. Retrieved August 1, 2024, from https://eso-stroke.org/antiphospholipid-syndrome-and-stroke/
- Nutescu, E. A., Burnett, A., Fanikos, J., Spinler, S., & Wittkowsky, A. (2016). Pharmacology of anticoagulants used in the treatment of venous thromboembolism. Journal of Thrombosis and Thrombolysis, 41, 15–31. https://doi.org/10.1007/s11239-015-1314-3
- Nutescu, E. A., Shapiro, N. L., Ibrahim, S., & West, P. (2006). Warfarin and its interactions with foods, herbs and other dietary supplements. Expert Opinion on Drug Safety, 5(3), 433–451. https://doi.org/10.1517/14740338.5.3.433
- Nutrition Source. (2023, March). Zinc. Harvard T.H. Chan School of Public Health. https://nutritionsource.hsph.harvard.edu/zinc/
- Office of Dietary Supplements. (2021, March 29). Vitamin K - Fact Sheet for Health Professionals. National Institutes of Health [NIH]. https://ods.od.nih.gov/factsheets/VitaminK-HealthProfessional/
- Ojha, N., & Dhamoon, A. S. (2023, August 8). Myocardial Infarction. In StatPearls [Internet]. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK537076/
- Olas, B., Urbańska, K., & Bryś, M. (2020). Saponins as Modulators of the Blood Coagulation System and Perspectives Regarding Their Use in the Prevention of Venous Thromboembolic Incidents. Molecules, 25(21), 5171. https://doi.org/10.3390/molecules25215171
- Oleszek, M., & Oleszek, W. (2021). Saponins in Food. In J. Xiao, S. D. Sarker, & Y. Asakawa (Eds.), Handbook of Dietary Phytochemicals (pp. 1501–1540). Springer. https://doi.org/10.1007/978-981-15-4148-3_34
- Ornstein, D. L., & Cushman, M. (2003). Factor V Leiden. Circulation, 107(15), e94–e97. https://doi.org/10.1161/01.CIR.0000068167.08920.F1
- Osula, S., Bell, G. M., & Hornung, R. S. (2002). Acute myocardial infarction in young adults: Causes and management. Postgraduate Medical Journal, 78(915), 27–30. https://doi.org/10.1136/pmj.78.915.27
- Palta, S., Saroa, R., & Palta, A. (2014). Overview of the coagulation system. Indian Journal of Anaesthesia, 58(5), 515. https://doi.org/10.4103/0019-5049.144643
- Pastori, D., Menichelli, D., Cammisotto, V., & Pignatelli, P. (2021). Use of Direct Oral Anticoagulants in Patients With Antiphospholipid Syndrome: A Systematic Review and Comparison of the International Guidelines. Frontiers in Cardiovascular Medicine, 8. https://doi.org/10.3389/fcvm.2021.715878
- Pazzola, G., Zuily, S., & Erkan, D. (2015). The Challenge of Bleeding in Antiphospholipid Antibody-Positive Patients. Current Rheumatology Reports, 17(2), 7. https://doi.org/10.1007/s11926-014-0481-0
- Pengo, V., Biasiolo, A., Gresele, P., Marongiu, F., Erba, N., Veschi, F., Ghirarduzzi, A., Barcellona, D., & Tripodi, A. (2007). A Comparison of Lupus Anticoagulant–Positive Patients With Clinical Picture of Antiphospholipid Syndrome and Those Without. Arteriosclerosis, Thrombosis, and Vascular Biology, 27(12), e309–e310. https://doi.org/10.1161/ATVBAHA.107.153536
- Pengo, V., Bison, E., Banzato, A., Zoppellaro, G., Jose, S. P., & Denas, G. (2017). Lupus Anticoagulant Testing: Diluted Russell Viper Venom Time (dRVVT). In E. J. Favaloro & G. Lippi (Eds.), Hemostasis and Thrombosis: Methods and Protocols (pp. 169–176). Springer. https://doi.org/10.1007/978-1-4939-7196-1_14
- Pengo, V., Tripodi, A., Reber, G., Rand, J. H., Ortel, T. L., Galli, M., & De groot, P. G. (2009). Update of the guidelines for lupus anticoagulant detection. Journal of Thrombosis and Haemostasis, 7(10), 1737–1740. https://doi.org/10.1111/j.1538-7836.2009.03555.x
- Penn Medicine. (n.d.). Evaluating Blood Clots with Birth Control, Pregnancy, and HRT. Retrieved August 1, 2024, from https://www.pennmedicine.org/for-patients-and-visitors/find-a-program-or-service/hematology/blood-clotting-disorders/risk-assessment-birth-control-pregnancy-hrt
- Perry, S. L., Samsa, G. P., & Ortel, T. L. (2017). Point-of-care testing of the international normalized ratio in patients with antiphospholipid antibodies. Thrombosis and Haemostasis, 94, 1196–1202. https://doi.org/10.1160/TH05-06-0400
- Pichot, R., Watson, R. L., & Norton, I. T. (2013). Phospholipids at the Interface: Current Trends and Challenges. International Journal of Molecular Sciences, 14(6), Article 6. https://doi.org/10.3390/ijms140611767
- Pires da Rosa, G., Bettencourt, P., Rodríguez-Pintó, I., Cervera, R., & Espinosa, G. (2020). “Non-criteria” antiphospholipid syndrome: A nomenclature proposal. Autoimmunity Reviews, 19(12), 102689. https://doi.org/10.1016/j.autrev.2020.102689
- Pons-Estel, G. J., Andreoli, L., Scanzi, F., Cervera, R., & Tincani, A. (2017). The antiphospholipid syndrome in patients with systemic lupus erythematosus. Journal of Autoimmunity, 76, 10–20. https://doi.org/10.1016/j.jaut.2016.10.004
- Prashanth, P., Mukhaini, M., & Riyami, A. (2009). A Rare Presentation of Primary Antiphospholipid Syndrome. Oman Medical Journal, 24(4), 300–302. https://doi.org/10.5001/omj.2009.61
- Provenzale, J. M., Barboriak, D. P., Allen, N. B., & Ortel, T. L. (1998). Antiphospholipid antibodies: Findings at arteriography. American Journal of Neuroradiology, 19(4), 611–616. https://www.ajnr.org/content/19/4/611
- Qian, J., Chen, W., Wu, J., Lv, M., Jiang, S., Zeng, Z., Fang, Z., Chen, M., & Zhang, J. (2022). Effects and Mechanism of Action of Panax notoginseng Saponins on the Pharmacokinetics of Warfarin. European Journal of Drug Metabolism and Pharmacokinetics, 47(3), 331–342. https://doi.org/10.1007/s13318-022-00753-0
- Queremel Milani, D. A., & Davis, D. D. (2023, July 3). Pain Management Medications. In StatPearls [Internet]. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK560692/
- Radic, M., & Pattanaik, D. (2018). Cellular and Molecular Mechanisms of Anti-Phospholipid Syndrome. Frontiers in Immunology, 9, 969. https://doi.org/10.3389/fimmu.2018.00969
- Radin, M., Foddai, S. G., Cecchi, I., Rubini, E., Schreiber, K., Roccatello, D., Bertolaccini, M. L., & Sciascia, S. (2020). Antiphosphatidylserine/Prothrombin Antibodies: An Update on Their Association with Clinical Manifestations of Antiphospholipid Syndrome. Thrombosis and Haemostasis, 120, 592–598. https://doi.org/10.1055/s-0040-1705115
- Radin, M., Sciascia, S., Erkan, D., Pengo, V., Tektonidou, M. G., Ugarte, A., Meroni, P., Ji, L., Belmont, H. M., Cohen, H., Jesús, G. R. de, Branch, D. W., Fortin, P. R., Andreoli, L., Petri, M., Rodriguez, E., Rodriguez-Pinto, I., Knight, J. S., Atsumi, T., … Andrade, D. (2019). The adjusted global antiphospholipid syndrome score (aGAPSS) and the risk of recurrent thrombosis: Results from the APS ACTION cohort. Seminars in Arthritis and Rheumatism, 49(3), 464–468. https://doi.org/10.1016/j.semarthrit.2019.04.009
- Rand, J. H., & Wolgast, L. R. (2013). 20 - Antiphospholipid Syndrome: Pathogenesis, Clinical Presentation, Diagnosis, and Patient Management. In C. S. Kitchens, C. M. Kessler, & B. A. Konkle (Eds.), Consultative Hemostasis and Thrombosis (Third Edition) (pp. 324–341). W.B. Saunders. https://doi.org/10.1016/B978-1-4557-2296-9.00020-8
- Ranjan, P., Chakrawarty, A., Kumari, A., & Kumar, J. (2015). Immunization in Patients with Rheumatic Diseases: A Practical Guide for General Practitioners. Journal of Clinical and Diagnostic Research : JCDR, 9(5), OE01–OE04. https://doi.org/10.7860/JCDR/2015/14147.5972
- Rasool, Z. S., & Tiwari, V. (2023, July 17). Biochemistry, Lupus Anticoagulant. In StatPearls [Internet]. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK544357/
- Reed, M., Tadi, P., & Nicolas, D. (2023). Andexanet Alfa. In StatPearls [Internet]. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK519499/
- Rege, S., & Mackworth-Young, C. (2015). Antiphospholipid antibodies as biomarkers in psychiatry: Review of psychiatric manifestations in antiphospholipid syndrome. Translational Developmental Psychiatry, 3(1), 25452. https://doi.org/10.3402/tdp.v3.25452
- Reyes, N., & Abe, K. (2023, May 1). Deep Vein Thrombosis & Pulmonary Embolism | CDC Yellow Book 2024. CDC. https://wwwnc.cdc.gov/travel/yellowbook/2024/air-land-sea/deep-vein-thrombosis-and-pulmonary-embolism
- Ricarte, I. F., Dutra, L. A., Abrantes, F. F., Toso, F. F., Barsottini, O. G. P., Silva, G. S., de Souza, A. W. S., & Andrade, D. (2018). Neurologic manifestations of antiphospholipid syndrome. Lupus, 27(9), 1404–1414. https://doi.org/10.1177/0961203318776110
- Roche Diagnostics. (n.d.). CoaguChek® XS system. Retrieved August 1, 2024, from https://diagnostics.roche.com/global/en/products/instruments/coaguchek-xs-ins-804.html
- Rodríguez-Olleros Rodríguez, C., & Díaz Curiel, M. (2019). Vitamin K and Bone Health: A Review on the Effects of Vitamin K Deficiency and Supplementation and the Effect of Non-Vitamin K Antagonist Oral Anticoagulants on Different Bone Parameters. Journal of Osteoporosis, 2019, 2069176. https://doi.org/10.1155/2019/2069176
- Rodriguez-Pintó, I., Espinosa, G., & Cervera, R. (2024). What we know and what we don’t know about catastrophic antiphospholipid syndrome. Rheumatology, 63(SI), SI46–SI53. https://doi.org/10.1093/rheumatology/kead556
- Rodríguez-Pintó, I., Moitinho, M., Santacreu, I., Shoenfeld, Y., Erkan, D., Espinosa, G., & Cervera, R. (2016). Catastrophic antiphospholipid syndrome (CAPS): Descriptive analysis of 500 patients from the International CAPS Registry. Autoimmunity Reviews, 15(12), 1120–1124. https://doi.org/10.1016/j.autrev.2016.09.010
- Rolla, R., Vay, D., Mottaran, E., Parodi, M., Vidali, M., Sartori, M., Rigamonti, C., Bellomo, G., & Albano, E. (2001). Antiphospholipid antibodies associated with alcoholic liver disease specifically recognise oxidised phospholipids. Gut, 49(6), 852–859. https://doi.org/10.1136/gut.49.6.852
- Rosendaal, F. R., Helmerhorst, F. M., & Vandenbroucke, J. P. (2002). Female Hormones and Thrombosis. Arteriosclerosis, Thrombosis, and Vascular Biology, 22(2), 201–210. https://doi.org/10.1161/hq0202.102318
- Rosendaal, F. R., Van Hylckama Vlieg, A., Tanis, B. C., & Helmerhorst, F. M. (2003). Estrogens, progestogens and thrombosis. Journal of Thrombosis and Haemostasis, 1(7), 1371–1380. https://doi.org/10.1046/j.1538-7836.2003.00264.x
- Royal College of Psychiatrists. (n.d.). Neuropsychiatrist. Retrieved August 1, 2024, from https://www.rcpsych.ac.uk/become-a-psychiatrist/choose-psychiatry/what-is-psychiatry/types-of-psychiatrist/neuropsychiatry
- RxList Inc. (n.d.). Implanon. Retrieved August 1, 2024, from https://www.rxlist.com/implanon-drug.htm
- Şabanoğlu, C. (2021). The secret enemy during a flight: Economy class syndrome. Anatolian Journal of Cardiology, 25(Suppl 1), S13–S17. https://doi.org/10.5152/AnatolJCardiol.2021.S106
- Santacruz, J. C., Mantilla, M. J., Rueda, I., Pulido, S., Rodríguez, G., Londono, J., Devia, J. C. S., Ribero, M. J. M., Sr, I. R. C., Sr, S. P., Sr, G. R.-S., & Londono, J. (2022). Obstetric Antiphospholipid Syndrome From the Perspective of a Rheumatologist. Cureus, 14. https://doi.org/10.7759/cureus.21090
- Saponjski, J., Stojanovich, L., Petrovic, J., & Saponjski, D. (2017). The role of MSCT angiography in early detection of lower limb arterial lesions in patients with antiphospholipid syndrome. Immunologic Research, 65(2), 482–486. https://doi.org/10.1007/s12026-016-8887-6
- Schreiber, K., & Hunt, B. J. (2019). Managing antiphospholipid syndrome in pregnancy. Thrombosis Research, 181, S41–S46. https://doi.org/10.1016/S0049-3848(19)30366-4
- Sciascia, S., Sanna, G., Khamashta, M. A., Cuadrado, M. J., Erkan, D., Andreoli, L., & Bertolaccini, M. L. (2015). The estimated frequency of antiphospholipid antibodies in young adults with cerebrovascular events: A systematic review. Annals of the Rheumatic Diseases, 74(11), 2028–2033. https://doi.org/10.1136/annrheumdis-2014-205663
- Scoble, T., Wijetilleka, S., & Khamashta, M. A. (2011). Management of refractory anti-phospholipid syndrome. Autoimmunity Reviews, 10(11), 669–673. https://doi.org/10.1016/j.autrev.2011.04.030
- Serrano, M., Espinosa, G., Serrano, A., & Cervera, R. (2022). COVID-19 and the antiphospholipid syndrome. Autoimmunity Reviews, 21(12), 103206. https://doi.org/10.1016/j.autrev.2022.103206
- Shen, H., Huang, X., & Fan, C. (2021). Clinical Characteristics and Management of Cerebral Venous Sinus Thrombosis in Patients With Antiphospholipid Syndrome: A Single-Center Retrospective Study. Clinical and Applied Thrombosis/Hemostasis, 27, 1076029621999104. https://doi.org/10.1177/1076029621999104
- Shi, H., Teng, J., Sun, Y., Wu, X., Hu, Q., Liu, H., Cheng, X., Yin, Y., Ye, J., Chen, P. P., & Yang, C. (2017). Clinical characteristics and laboratory findings of 252 Chinese patients with anti-phospholipid syndrome: Comparison with Euro-Phospholipid cohort. Clinical Rheumatology, 36(3), 599–608. https://doi.org/10.1007/s10067-017-3549-1
- Shoenfeld, Y., Blank, M., Cervera, R., Font, J., Raschi, E., & Meroni, P. (2006). Infectious origin of the antiphospholipid syndrome. Annals of the Rheumatic Diseases, 65(1), 2–6. https://doi.org/10.1136/ard.2005.045443
- Signorelli, F., Balbi, G. G. M., Domingues, V., & Levy, R. A. (2018). New and upcoming treatments in antiphospholipid syndrome: A comprehensive review. Pharmacological Research, 133, 108–120. https://doi.org/10.1016/j.phrs.2018.04.012
- Siller-Matula, J. M., Schwameis, M., Blann, A., Mannhalter, C., & Jilma, B. (2017). Thrombin as a multi-functional enzyme. Thrombosis and Haemostasis, 106, 1020–1033. https://doi.org/10.1160/TH10-11-0711
- Silver, N., & Fischer-Baum, R. (2014, December 4). Which City Has The Most Unpredictable Weather? FiveThirtyEight. https://fivethirtyeight.com/features/which-city-has-the-most-unpredictable-weather/
- Silver, R. M., Parker, C. B., Reddy, U. M., Goldenberg, R., Coustan, D., Dudley, D. J., Saade, G. R., Stoll, B., Koch, M. A., Conway, D., Bukowski, R., Rowland Hogue, C. J., Pinar, H., Moore, J., Willinger, M., & Branch, D. W. (2013). Antiphospholipid Antibodies in Stillbirth. Obstetrics & Gynecology, 122(3), 641. https://doi.org/10.1097/AOG.0b013e3182a1060e
- Simes, D. C., Viegas, C. S. B., Araújo, N., & Marreiros, C. (2020). Vitamin K as a Diet Supplement with Impact in Human Health: Current Evidence in Age-Related Diseases. Nutrients, 12(1), Article 1. https://doi.org/10.3390/nu12010138
- Soybilgic, A., Aguiar, C. L., Massicotte, M. P., Kenet, G., Yeh, E. A., Andreoli, L., Avcin, T., & Myones, B. L. (2017). 15th International Congress on Antiphospholipid Antibodies Task Force on Pediatric Antiphospholipid Syndrome Report. In D. Erkan & M. D. Lockshin (Eds.), Antiphospholipid Syndrome: Current Research Highlights and Clinical Insights (pp. 291–306). Springer International Publishing. https://doi.org/10.1007/978-3-319-55442-6_16
- Stoots, S. A., Lief, L., & Erkan, D. (2019). Clinical Insights into Diffuse Alveolar Hemorrhage in Antiphospholipid Syndrome. Current Rheumatology Reports, 21(10), 56. https://doi.org/10.1007/s11926-019-0852-7
- Stosic, M., Ambrus, J., Garg, N., Weinstock-Guttman, B., Ramanathan, M., Kalman, B., Minagar, A., Munschauer, F. E., Galey, T. M., Hussein, S., Bakshi, R., & Zivadinov, R. (2010). MRI characteristics of patients with antiphospholipid syndrome and multiple sclerosis. Journal of Neurology, 257(1), 63–71. https://doi.org/10.1007/s00415-009-5264-6
- Suvajac, G., Stojanovich, L., & Milenkovich, S. (2007). Ocular manifestations in antiphospholipid syndrome. Autoimmunity Reviews, 6(6), 409–414. https://doi.org/10.1016/j.autrev.2006.11.005
- Sweis, R. N., & Jivan, A. (2024, February). Acute Myocardial Infarction (MI). MSD Manual Professional Edition. https://www.msdmanuals.com/en-sg/professional/cardiovascular-disorders/coronary-artery-disease/acute-myocardial-infarction-mi
- Takahashi, H., & Echizen, H. (2003). Pharmacogenetics of CYP2C9 and interindividual variability in anticoagulant response to warfarin. The Pharmacogenomics Journal, 3(4), 202–214. https://doi.org/10.1038/sj.tpj.6500182
- Tan, B., Thong, B., Shivananda, S., Han, W., & Chng, H. (2009). Clinical manifestations and outcomes of antithrombotic treatment of the Tan Tock Seng Hospital Singapore antiphospholipid syndrome cohort. Lupus, 18(8), 752–758. https://doi.org/10.1177/0961203309103303
- Taylor, J. R., Richter, C., Lindamood, C., Liu, X., Zumberg, M., & Fletcher, B. (2017). Accuracy of CoaguChek XS in Patients With Antiphospholipid Syndrome. Point of Care, 16(4), 161. https://doi.org/10.1097/POC.0000000000000149
- Thomas, S. (2024, March 8). How Long Does Alcohol Stay in Your System? American Addiction Centers. https://americanaddictioncenters.org/alcohol/how-long-in-system
- Tohidi-Esfahani, I., Mittal, P., Isenberg, D., Cohen, H., & Efthymiou, M. (2024). Platelets and Thrombotic Antiphospholipid Syndrome. Journal of Clinical Medicine, 13(3), Article 3. https://doi.org/10.3390/jcm13030741
- Truglia, S., Capozzi, A., Mancuso, S., Manganelli, V., Rapino, L., Riitano, G., Recalchi, S., Colafrancesco, S., Ceccarelli, F., Garofalo, T., Alessandri, C., Longo, A., Misasi, R., Conti, F., & Sorice, M. (2022). Relationship Between Gender Differences and Clinical Outcome in Patients With the Antiphospholipid Syndrome. Frontiers in Immunology, 13. https://doi.org/10.3389/fimmu.2022.932181
- Truglia, S., Mancuso, S., Capozzi, A., Recalchi, S., Riitano, G., Longo, A., De Carolis, S., Spinelli, F. R., Alessandri, C., Ceccarelli, F., De Carolis, C., Misasi, R., Sorice, M., & Conti, F. (2022). ‘Non-criteria antiphospholipid antibodies’: Bridging the gap between seropositive and seronegative antiphospholipid syndrome. Rheumatology, 61(2), 826–833. https://doi.org/10.1093/rheumatology/keab414
- Tubek, S., Grzanka, P., & Tubek, I. (2008). The Role of Zinc in Thrombosis and Pulmonary Embolism in the Course of Antiphospholipid Syndrome (APS)—Short Review. Biological Trace Element Research, 122(3), 193–196. https://doi.org/10.1007/s12011-007-8077-4
- Udayangani, S. (2022, December 12). What is the Difference Between Factor V Leiden and Antiphospholipid Syndrome. Difference Between. https://www.differencebetween.com/what-is-the-difference-between-factor-v-leiden-and-antiphospholipid-syndrome/
- University of Rochester Medical Center. (n.d.-a). Cardiolipin Antibody. Retrieved August 1, 2024, from https://www.urmc.rochester.edu/encyclopedia/content.aspx?contenttypeid=167&contentid=cardiolipin_antibody
- University of Rochester Medical Center. (n.d.-b). Overview of the Vascular System. Retrieved August 1, 2024, from https://www.urmc.rochester.edu/encyclopedia/content.aspx?contenttypeid=85&contentid=P08254
- UpToDate, Inc. (n.d.). Medications that interfere with the effect of warfarin. Retrieved August 1, 2024, from https://www.uptodate.com/contents/image?imageKey=HEME%2F62697
- U.S. Food & Drug Administration [FDA]. (2018). Generic Enoxaparin Questions and Answers. https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/generic-enoxaparin-questions-and-answers
- Vaccarino, A., Pagliaro, M., Rollone, C., Melis, F., De Marco, F., Savio, K., Guido, M., Bazzan, M., Imperiale, D., & Pini, M. (2019). Prevalence of the Antiphospholipid Antibodies in Young Adults with Ischemic Stroke. Blood, 134, 4952. https://doi.org/10.1182/blood-2019-123727
- van der Linden, J., Almskog, L., Liliequist, A., Grip, J., Fux, T., Rysz, S., Ågren, A., Oldner, A., & Ståhlberg, M. (2020). Thromboembolism, Hypercoagulopathy, and Antiphospholipid Antibodies in Critically Ill Coronavirus Disease 2019 Patients: A Before and After Study of Enhanced Anticoagulation. Critical Care Explorations, 2(12), e0308. https://doi.org/10.1097/CCE.0000000000000308
- Wang, T., Zhou, H., Xie, H., Mu, Y., Xu, Y., Liu, J., & Zhang, X. (2014). Epigallocatechin-3-gallate inhibits TF and TNF-α expression induced by the anti-β2GPI/β2GPI complex in human THP-1 cells. International Journal of Molecular Medicine, 33(4), 994–1002. https://doi.org/10.3892/ijmm.2014.1635
- Wong, R. W. S., Chan, J. K. H., & Wong, K. L. (1987). Lupus Anticoagulant—A Double Misnomer. Asian Pacific Journal of Allergy and Immunology, 5, 161–165. https://www.apjai-journal.org/wp-content/uploads/2017/12/10LupusAnticoagulantAPJAIVol5No2December1987P161.pdf
- Yang, Y., Jiang, H., Tang, Z., Pan, H., Liu, H., Cheng, X., Su, Y., Ye, J., Hu, Q., Meng, J., Chi, H., Zhou, Z., Jia, J., Yang, C., Shi, H., Teng, J., & Liu, T. (2024). Assessment of the 2023 ACR/EULAR antiphospholipid syndrome classification criteria in a Chinese cohort: Impact on clinical practice. Journal of Autoimmunity, 146, 103237. https://doi.org/10.1016/j.jaut.2024.103237
- Yelnik, C. M., Kozora, E., & Appenzeller, S. (2016). Non-stroke Central Neurologic Manifestations in Antiphospholipid Syndrome. Current Rheumatology Reports, 18(2), 11. https://doi.org/10.1007/s11926-016-0568-x
- Yokoyama, S., Ieda, S., Nagano, M., Nakagawa, C., Iwase, M., Hosomi, K., & Takada, M. (2020). Association between oral anticoagulants and osteoporosis: Real-world data mining using a multi-methodological approach. International Journal of Medical Sciences, 17(4), 471–479. https://doi.org/10.7150/ijms.39523
- Zhao, Z., Zhao, F., Wang, X., Liu, D., Liu, J., Zhang, Y., Hu, X., Zhao, M., Tian, C., Dong, S., & Jin, P. (2023). Genetic Factors Influencing Warfarin Dose in Han Chinese Population: A Systematic Review and Meta-Analysis of Cohort Studies. Clinical Pharmacokinetics, 62(6), 819–833. https://doi.org/10.1007/s40262-023-01258-y